

Magnetic resonance imaging adds prognostic value to EEG after pediatric cardiac arrest
- PMID: 35227820
- PMCID: PMC9001021
- DOI: 10.1016/j.resuscitation.2022.02.017
Magnetic resonance imaging adds prognostic value to EEG after pediatric cardiac arrest
Abstract
Aim: To investigate how combined electrographic and radiologic data inform outcomes in children after cardiac arrest.
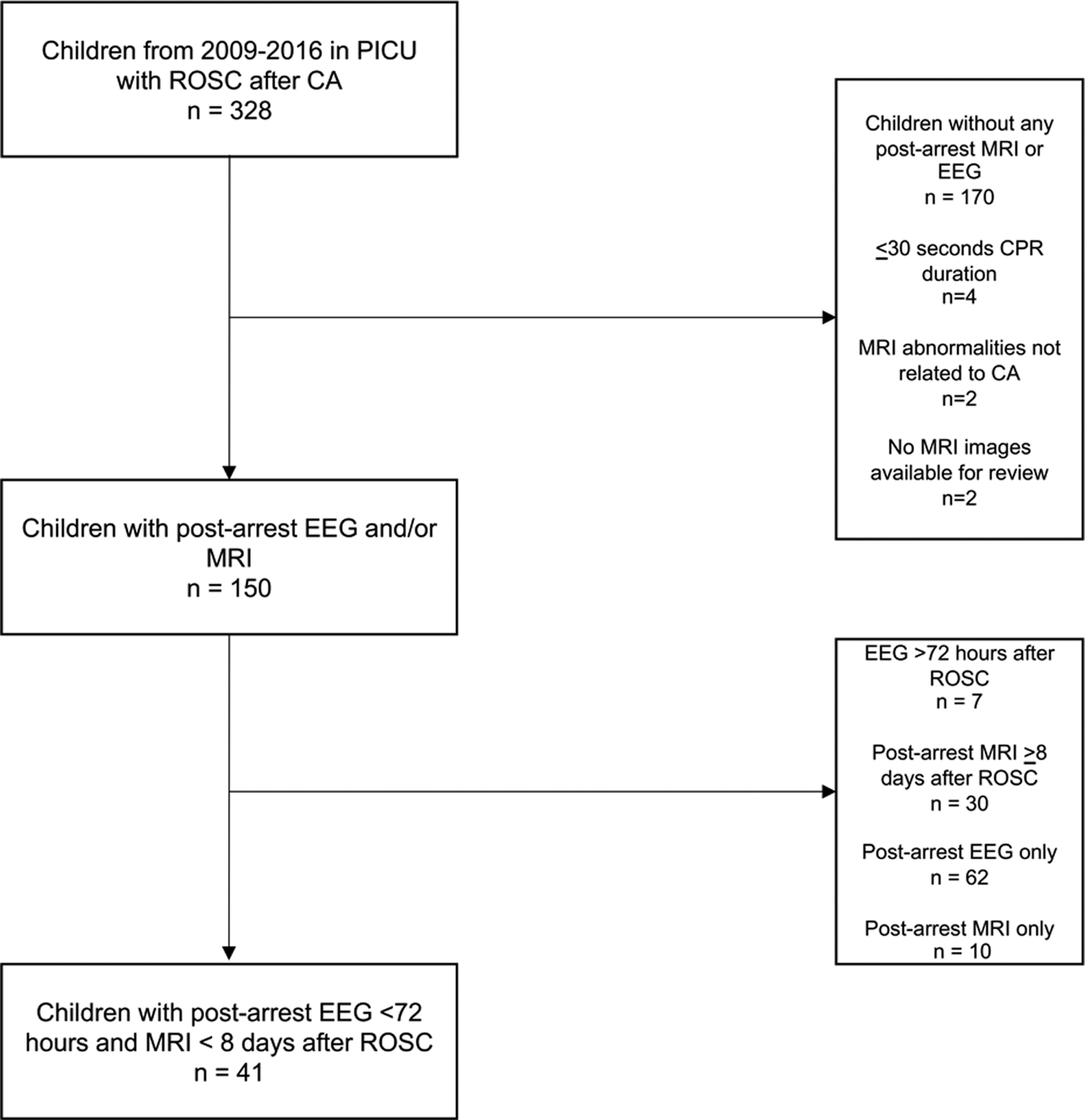
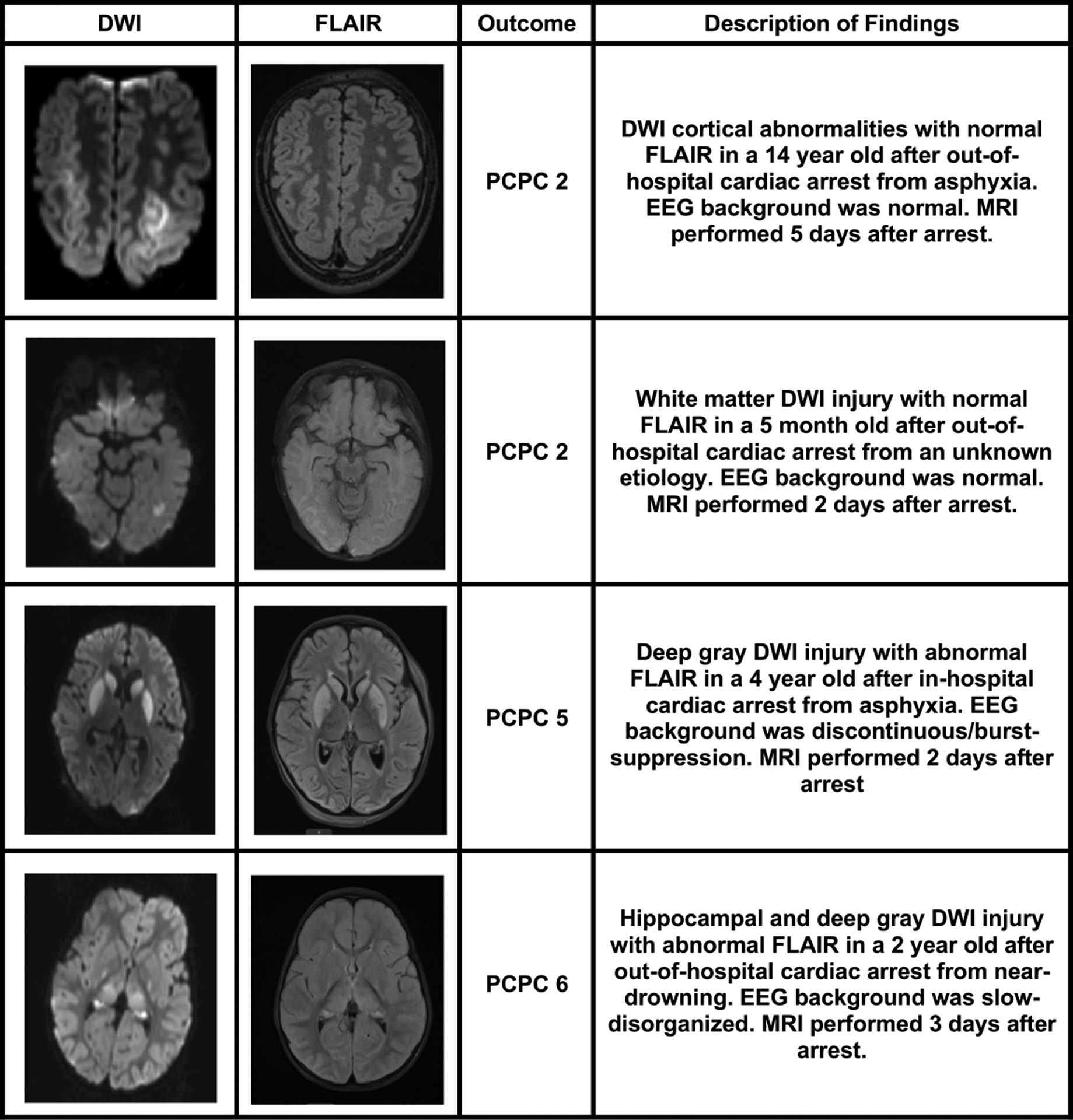
Methods: Retrospective observational study of children admitted to the pediatric intensive care unit (PICU) of a tertiary children's hospital with diagnosis of cardiac arrest from 2009 to 2016. The first 20 min of electroencephalogram (EEG) background was blindly scored. Presence and location of magnetic resonance imaging (MRI) diffusion-weighted image (DWI) abnormalities were correlated with T2-weighted signal. Outcomes were categorized using Pediatric Cerebral Performance Category (PCPC) scores at hospital discharge, with "poor outcome" reflecting a PCPC score of 4-6. Logistic regression models examined the association of EEG and MRI variables with outcome.
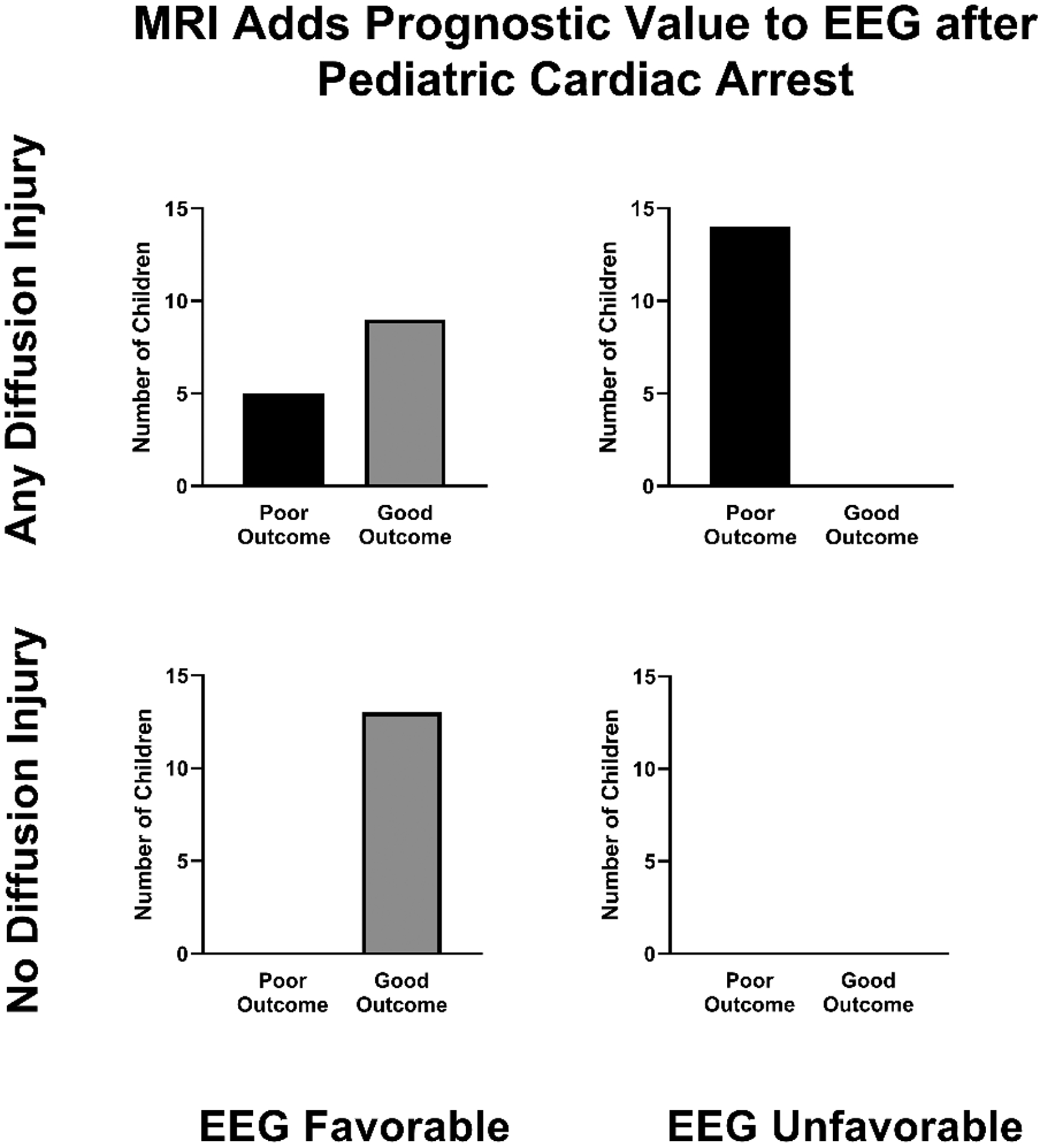
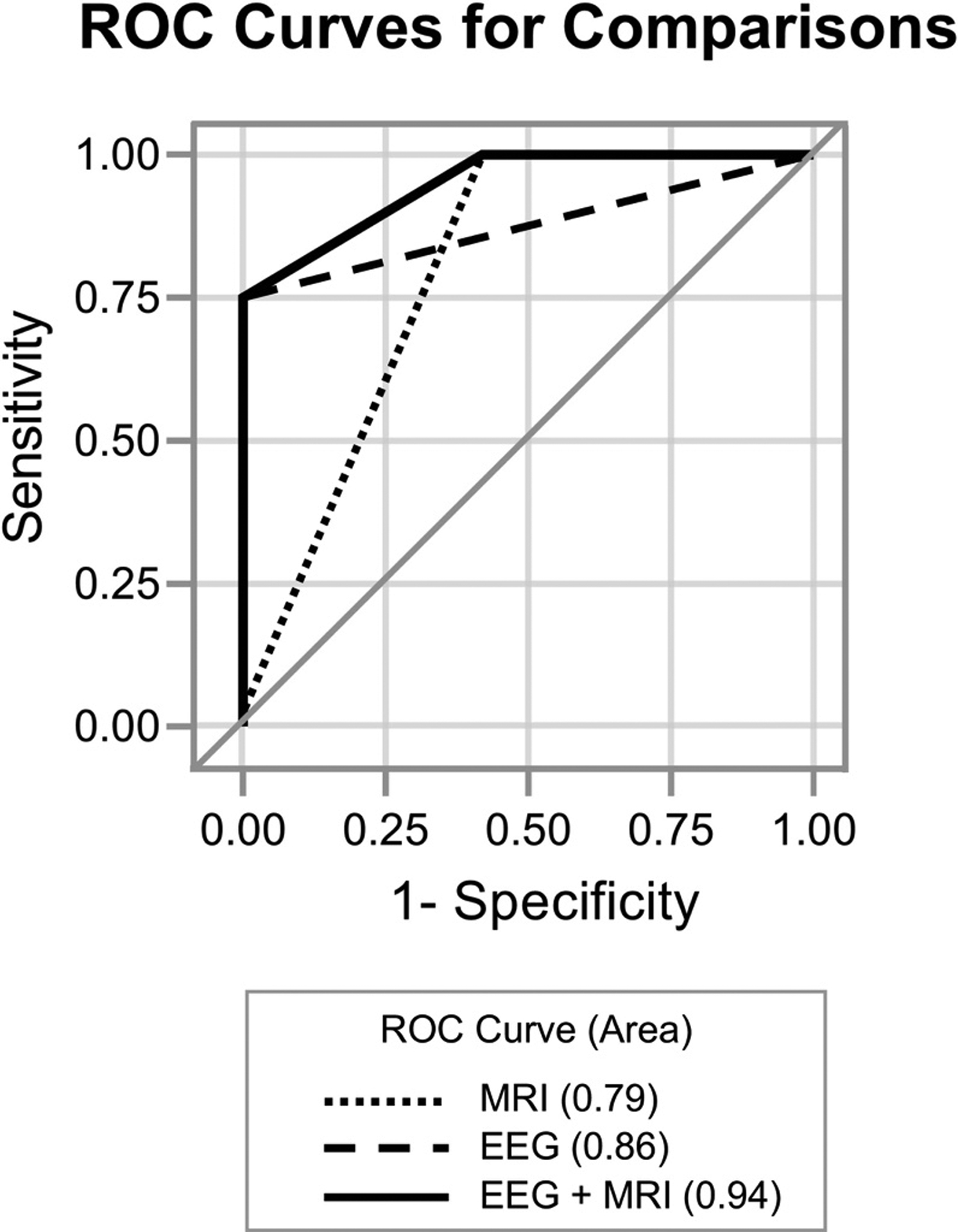
Results: 41 children met inclusion criteria and had both post-arrest EEG monitoring within 72 hours after ROSC and brain MRI performed within 8 days. Among the 19 children with poor outcome, 10 children did not survive to discharge. Severely abnormal EEG background (p < 0.0001) and any diffusion restriction (p < 0.0001) were associated with poor outcome. The area under the ROC curve (AUC) for identifying outcome based on EEG background alone was 0.86, which improved to 0.94 with combined EEG and MRI data (p = 0.02).
Conclusion: Diffusion abnormalities on MRI within 8 days after ROSC add to the prognostic value of EEG background in children surviving cardiac arrest.
Keywords: EEG; MRI; Outcome; Pediatric cardiac arrest.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
