

Humoral immune responses to COVID-19 vaccination in people living with HIV receiving suppressive antiretroviral therapy
- PMID: 35228535
- PMCID: PMC8885829
- DOI: 10.1038/s41541-022-00452-6
Humoral immune responses to COVID-19 vaccination in people living with HIV receiving suppressive antiretroviral therapy
Abstract
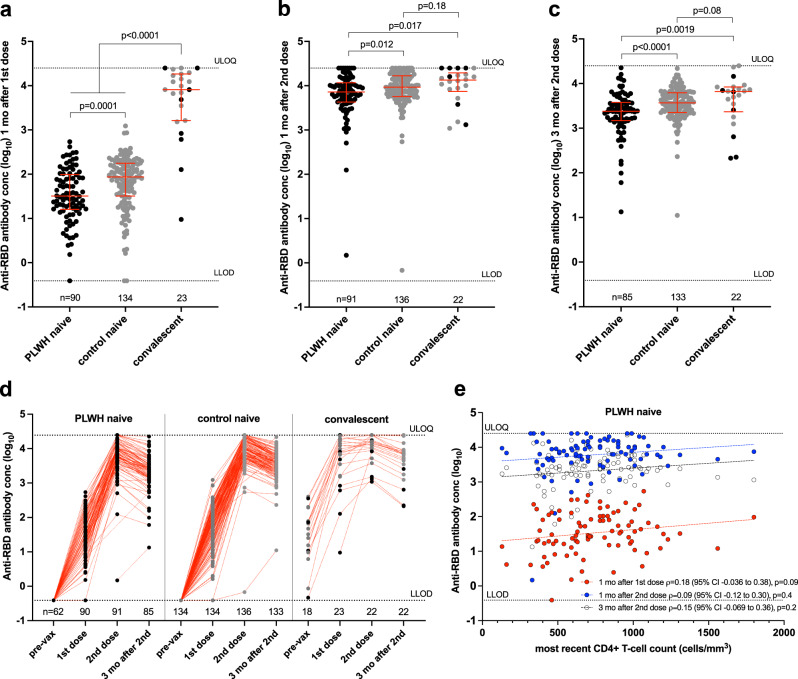
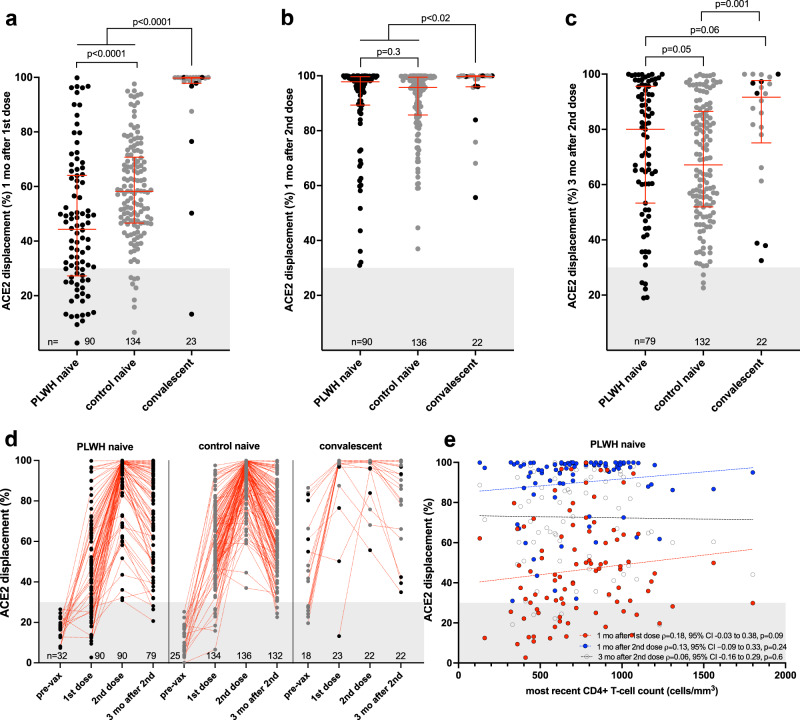
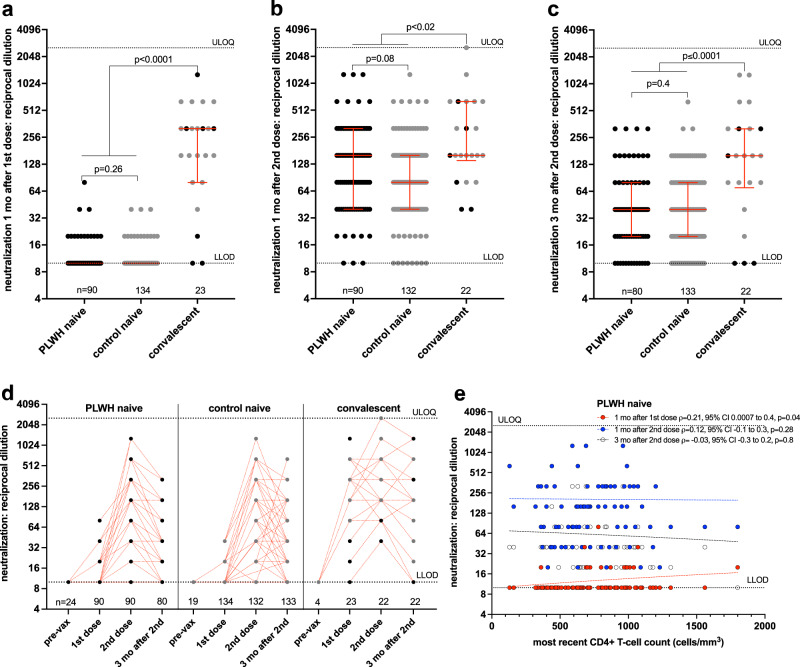
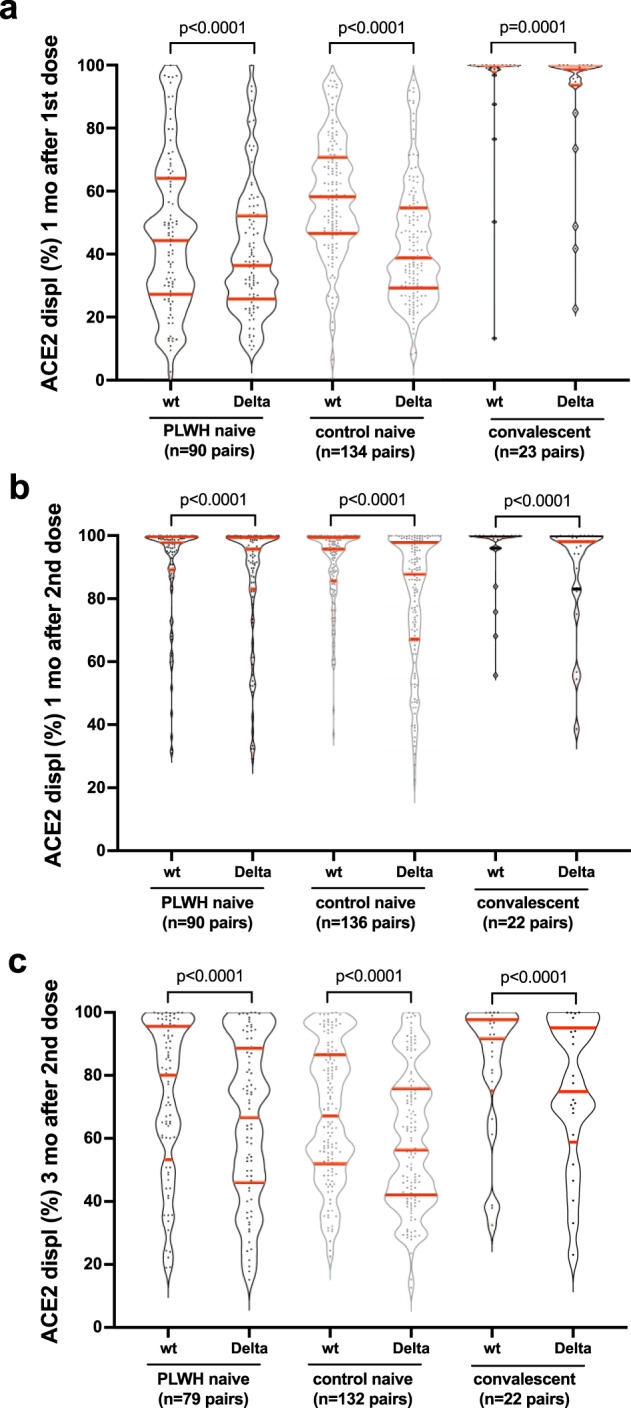
Humoral responses to COVID-19 vaccines in people living with HIV (PLWH) remain incompletely characterized. We measured circulating antibodies against the SARS-CoV-2 spike protein receptor-binding domain (RBD), ACE2 displacement and viral neutralization activities one month following the first and second COVID-19 vaccine doses, and again 3 months following the second dose, in 100 adult PLWH and 152 controls. All PLWH were receiving suppressive antiretroviral therapy, with median CD4+ T-cell counts of 710 (IQR 525-935) cells/mm3, though nadir CD4+ T-cell counts ranged as low as <10 cells/mm3. After adjustment for sociodemographic, health and vaccine-related variables, HIV infection was associated with lower anti-RBD antibody concentrations and ACE2 displacement activity after one vaccine dose. Following two doses however, HIV was not significantly associated with the magnitude of any humoral response after multivariable adjustment. Rather, older age, a higher burden of chronic health conditions, and dual ChAdOx1 vaccination were associated with lower responses after two vaccine doses. No significant correlation was observed between recent or nadir CD4+ T-cell counts and responses to two vaccine doses in PLWH. These results indicate that PLWH with well-controlled viral loads and CD4+ T-cell counts in a healthy range generally mount strong initial humoral responses to dual COVID-19 vaccination. Factors including age, co-morbidities, vaccine brand, response durability and the rise of new SARS-CoV-2 variants will influence when PLWH will benefit from additional doses. Further studies of PLWH who are not receiving antiretroviral treatment or who have low CD4+ T-cell counts are needed, as are longer-term assessments of response durability.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Humoral immune responses to COVID-19 vaccination in people living with HIV receiving suppressive antiretroviral therapy.medRxiv [Preprint]. 2021 Oct 15:2021.10.03.21264320. doi: 10.1101/2021.10.03.21264320. medRxiv. 2021. Update in: NPJ Vaccines. 2022 Feb 28;7(1):28. doi: 10.1038/s41541-022-00452-6. PMID: 34671779 Free PMC article. Updated. Preprint.
References
-
- BC Centre for Excellence in HIV/AIDS Committee on Drug Evaluation and Therapy. Committee Statement Update on the use of COVID-19 Vaccines in Persons Living with HIVhttp://bccfe.ca/therapeutic-guidelines/bc-cfe-cdet-statement-use-of-covi... (2021).
Grants and funding
- R01AI134229/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- VAC-009/Genome British Columbia
- Scholar Award/Michael Smith Foundation for Health Research (MSFHR)
- VAC-009/Michael Smith Foundation for Health Research (MSFHR)
- VAC-009/BCCDC Foundation for Public Health (BCCDC Foundation for Population and Public Health)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
