

Influence of hospital capabilities and prehospital time on outcomes of thrombectomy for stroke in Japan from 2013 to 2016
- PMID: 35228551
- PMCID: PMC8885934
- DOI: 10.1038/s41598-022-06074-1
Influence of hospital capabilities and prehospital time on outcomes of thrombectomy for stroke in Japan from 2013 to 2016
Abstract
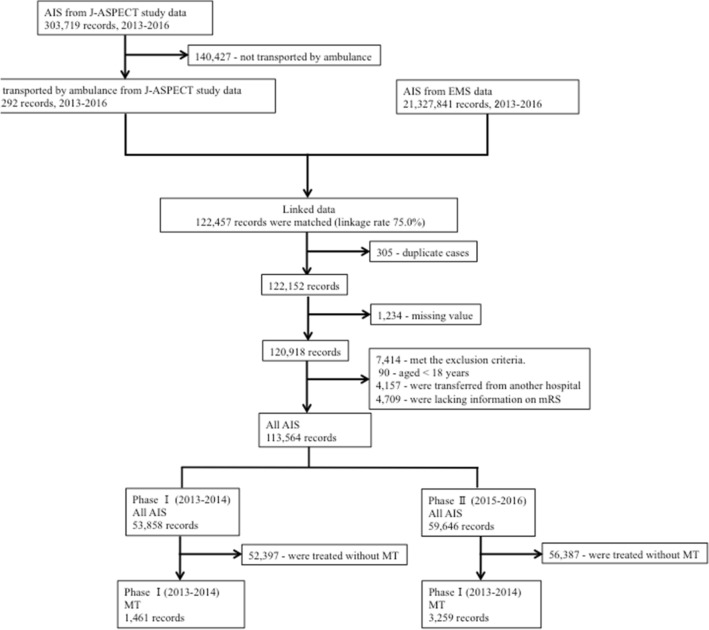
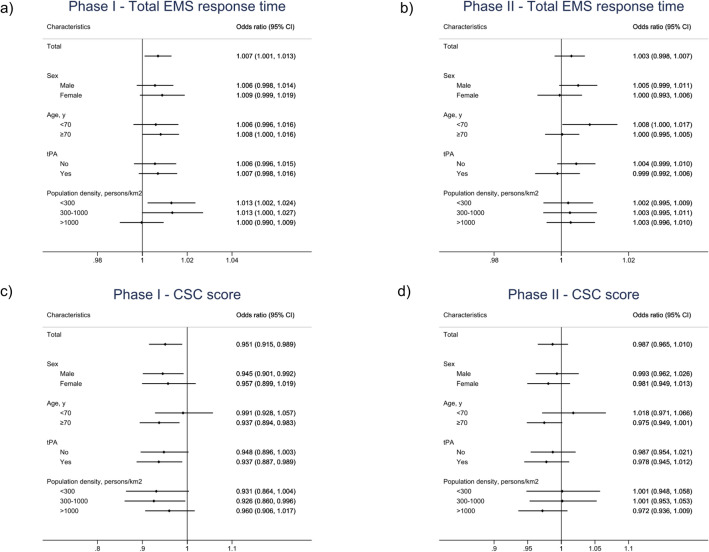
To determine whether increasing thrombectomy-capable hospitals with moderate comprehensive stroke center (CSC) capabilities is a valid alternative to centralization of those with high CSC capabilities. This retrospective, nationwide, observational study used data from the J-ASPECT database linked to national emergency medical service (EMS) records, captured during 2013-2016. We compared the influence of mechanical thrombectomy (MT) use, the CSC score, and the total EMS response time on the modified Rankin Scale score at discharge among patients with acute ischemic stroke transported by ambulance, in phases I (2013-2014, 1461 patients) and II (2015-2016, 3259 patients). We used ordinal logistic regression analyses to analyze outcomes. From phase I to II, MTs increased from 2.7 to 5.5%, and full-time endovascular physicians per hospital decreased. The CSC score and EMS response time remained unchanged. In phase I, higher CSC scores were associated with better outcomes (1-point increase, odds ratio [95% confidence interval]: 0.951 [0.915-0.989]) and longer EMS response time was associated with worse outcomes (1-min increase, 1.007 [1.001-1.013]). In phase II, neither influenced the outcomes. During the transitional shortage of thrombectomy-capable hospitals, increasing hospitals with moderate CSC scores may increase nationwide access to MT, improving outcomes.
© 2022. The Author(s).
Conflict of interest statement
Dr. Iihara is the principal investigator. Dr. Kada reports receiving personal fees from Bayer Yakuhin, Ltd. outside of the submitted work. Dr. Hagihara reports receiving a KAKENHI grant from the Japan Society for the Promotion of Science and grants from the Japan Agency for Medical Research and Development during the conduct of the study. Dr. Nishimura reports receiving grants from the Japanese Ministry of Health, Labour and Welfare and the Japan Agency for Medical Research and Development during the conduct of the study. Dr. Kitazono reports receiving grants from the Japanese Ministry of Health, Labour and Welfare and the Japan Agency for Medical Research and Development during the conduct of the study; personal fees from Bayer Yakuhin, Ltd., Daiichi Sankyo Co., Ltd., and Chugai Pharmaceutical Co., Ltd.; and grants from Takeda Pharmaceuticals Co., Ltd., Daiichi Sankyo Co., Ltd., Mitsubishi Tanabe Pharma Co, Eisai Co., Ltd., Astellas Pharma Inc., Chugai Pharmaceutical Co., Ltd., and MSD KK, outside of the submitted work. Dr. Ohta reports receiving funding for travel to speak at conference, Takeda Pharmaceutical, Tanabe Mitsubishi, Daiichi Sankyo, Otsuka Pharmaceutical, Stryker, Bayer, Kaneka, MSD, Medicos Hirata, Kyorin Pharmaceutical, Kochi Prefecture Kidney bank society, Uji Tokushukai Hospital, The Japanese Congress of Neurological Surgeons, Eisai, Medtronic and Terumo. He also reports Speakers' Bureaus, Takeda Pharmaceutical , Tanabe Mitsubishi, Daiichi Sankyo, Otsuka Pharmaceutical, Stryker, Bayer, Kaneka, MSD, Medicos Hirata, Kyorin Pharmaceutical , Kochi Prefecture Kidney bank society , Uji Tokushukai Hospital, Eisai, Medtronic and Terumo. Dr. Sakai reports receiving grants from Terumo Co., Ltd. and Daiichi Sankyo Co., Ltd.; and personal fees from Biomedical Solutions Co., Ltd., Johnson and Johnson Co., Ltd., Medtronic Co., Ltd., Penumbra Co., Ltd., Stryker Co., Ltd., and Terumo Co., Ltd., outside of the submitted work. Dr. Higashi reports receiving grants from the Japan Agency for Medical Research and Development and a KAKENHI grant from the Japan Society for the Promotion of Science during the conduct of the study. Dr. Sakamoto reports receiving grants from the Japan Agency for Medical Research and Development during the conduct of the study; personal fees from Boehringer Ingelheim Japan, Inc.; and grants from Asahi Kasei Pharma Corporation, Japan Blood Products Organization, and the Japanese Ministry of Health, Labour and Welfare, outside the submitted work. Dr. Iihara reports receiving grants from the Japanese Ministry of Health, Labour and Welfare, the Japan Agency for Medical Research and Development, and a KAKENHI grant from the Japan Society for the Promotion of Science during the conduct of the study; as well as grants from Otsuka Pharmaceutical Co., Ltd., Kaneka Medix Corporation, Eisai Co., Ltd., and Mitsubishi Tanabe Pharma Co., outside the submitted work. All other authors have nothing to disclose.
Figures

References
-
- Kada, A. et al. National trends in outcomes of ischemic stroke and prognostic influence of stroke center capability in Japan, 2010–2016. Int. J. Stroke; doi:10.1177/1747493019884526 (2019). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
