

Treatment with glucagon-like peptide-1 receptor agonists and incidence of dementia: Data from pooled double-blind randomized controlled trials and nationwide disease and prescription registers
- PMID: 35229024
- PMCID: PMC8864443
- DOI: 10.1002/trc2.12268
Treatment with glucagon-like peptide-1 receptor agonists and incidence of dementia: Data from pooled double-blind randomized controlled trials and nationwide disease and prescription registers
Abstract
Introduction: People with type 2 diabetes have increased risk of dementia. Glucagon-like peptide-1 (GLP-1) receptor agonists (RAs) are among the promising therapies for repurposing as a treatment for Alzheimer's disease; a key unanswered question is whether they reduce dementia incidence in people with type 2 diabetes.
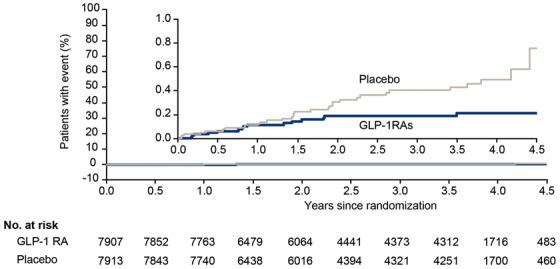
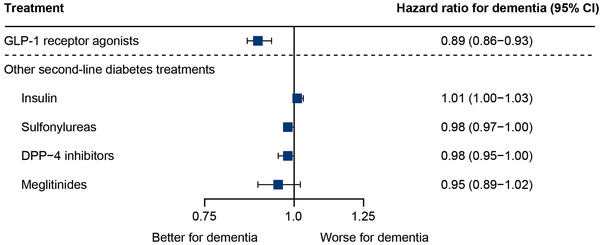
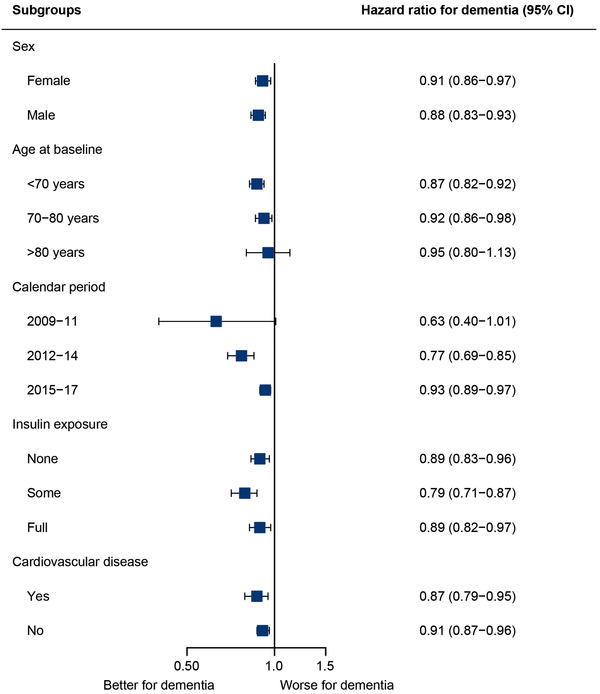
Methods: We assessed exposure to GLP-1 RAs in patients with type 2 diabetes and subsequent diagnosis of dementia in two large data sources with long-term follow-up: pooled data from three randomized double-blind placebo-controlled cardiovascular outcome trials (15,820 patients) and a nationwide Danish registry-based cohort (120,054 patients).
Results: Dementia rate was lower both in patients randomized to GLP-1 RAs versus placebo (hazard ratio [HR]: 0.47 (95% confidence interval [CI]: 0.25-0.86) and in the nationwide cohort (HR: 0.89; 95% CI: 0.86-0.93 with yearly increased exposure to GLP-1 RAs).
Discussion: Treatment with GLP-1 RAs may provide a new opportunity to reduce the incidence of dementia in patients with type 2 diabetes.
Keywords: dementia; glucagon‐like peptide‐1 receptor agonists; randomized controlled trial; real‐world evidence; type 2 diabetes.
© 2022 The Authors. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring published by Wiley Periodicals, LLC on behalf of Alzheimer's Association.
Conflict of interest statement
CHN, TG, EH, and CTP report no conflicts of interests. SF reports grants from Novo Nordisk related to the manufacture of GLP‐1 RAs during the conduct of the study and support for attending meetings and/or travel from the German Research Foundation (payments made to institution); she has also been secretary of the German Consortium in Statistics (DAGStat). CTMH, DVM, KK are Novo Nordisk employees and report personal fees from Novo Nordisk A/S related to the manufacture of GLP‐1 RAs (salary and shareholder), during the conduct of the study. KK also reports Novo Nordisk stock in pension funds. CTMH is also inventor on a patent application related to GLP‐1 compounds and indications (patent is owned by Novo Nordisk and she receives no financial or other benefits from it) and is a minor stockholder of Novo Nordisk A/S. CB reports grants and personal fees from Acadia, Addex, Exciva, Janssen, Suven, and Lundbeck; personal fees from Roche, Otsuka, Biogen, Eli Lilly, Sunovion, Novo Nordisk, and AARP; grants and personal fees from Synexus, outside the submitted work; he also reports the following grants to his institution (UoE) from: 2021 ADDF, 2020 UKRI, 2019 IMI2, NIH, Charles Wolfson Foundation, Novo Nordisk, 2018 MRC, Synexus, Capital, award from Dennis and Mireille Gillings Foundation, Novartis, and Oryzon; honoraria from Harvard University (to institution, UoE), GE Healthcare, Acadia, AARP, and Addex. LBK is a Novo Nordisk employee and an inventor on numerous patents and applications related to GLP‐1 compounds and indications; all patents are owned by Novo Nordisk, which markets liraglutide and semaglutide, and she receives no financial or other benefits from them. BZ reports grants and personal fees from Novo Nordisk during the conduct of the study, and personal fees from Eli Lilly, Merck, Boehringer Ingelheim, and Janssen, outside the submitted work. LSM is a Novo Nordisk employee and reports personal fees from Novo Nordisk A/S related to the manufacture of GLP‐1 RA (salary) during the conduct of the study; she is also vice chair of the Danish Society for Pharmacoepidemiology and is on the executive committee for the Nordic PharmacoEpidemiological Network.
Figures
References
-
- Prince M, Karagiannidou M, Comas‐Herrera A, Knapp M. World Alzheimer Report 2016. Improving healthcare for people living with dementia. Alzheimers Dis Int. 2016:1‐127. https://www.alzint.org/u/WorldAlzheimerReport2016.pdf.
-
- International Diabetes Federation. IDF Diabetes Atlas Ninth Edition 2019. 2019; - PubMed
LinkOut - more resources
Full Text Sources