

The next wave of cellular immunotherapies in pancreatic cancer
- PMID: 35229033
- PMCID: PMC8857655
- DOI: 10.1016/j.omto.2022.01.010
The next wave of cellular immunotherapies in pancreatic cancer
Abstract
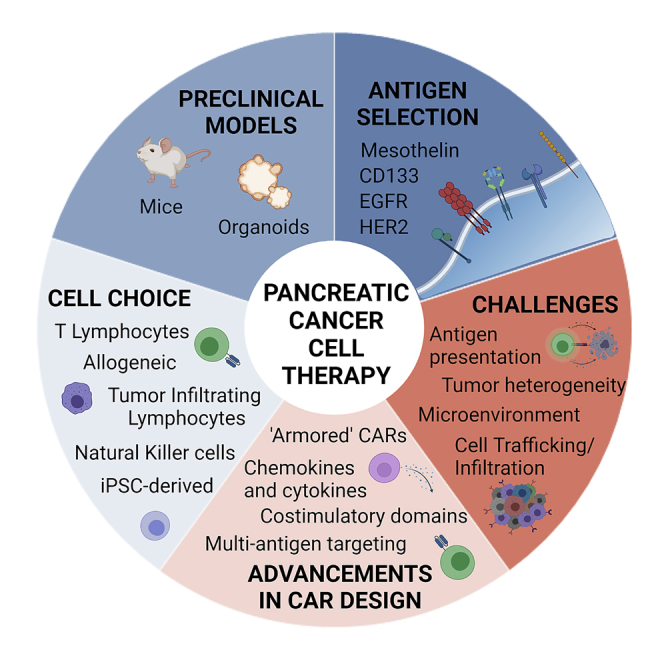
Pancreatic cancer is an aggressive disease that is predicted to become the second leading cause of cancer-related death worldwide by 2030. The overall 5-year survival rate is around 10%. Pancreatic cancer typically presents late with locally advanced or metastatic disease, and there are limited effective treatments available. Cellular immunotherapy, such as chimeric antigen receptor (CAR) T cell therapy, has had significant success in treating hematological malignancies. However, CAR T cell therapy efficacy in pancreatic cancer has been limited. This review provides an overview of current and ongoing CAR T cell clinical studies of pancreatic cancer and the major challenges and strategies to improve CAR T cell efficacy. These strategies include arming CAR T cells; developing off-the-shelf allogeneic CAR T cells; using other immune CAR cells, like natural killer cells and tumor-infiltrating lymphocytes; and combination therapy. Careful incorporation of preclinical models will enhance management of affected individuals, assisting incorporation of cellular immunotherapies. A multifaceted, personalized approach involving cellular immunotherapy treatment is required to improve pancreatic cancer outcomes.
Keywords: CAR T cell therapy; adoptive T cell therapy; cellular immunotherapy; checkpoint blockade; combination therapy; organoids; pancreatic cancer; preclinical models; tumor microenvironment.
Crown Copyright © 2022.
Conflict of interest statement
J.E.J.R. reports advisory roles in The Gene Technology Technical Advisory Committee, Office of the Gene Technology Regulator, Australian Government. J.E.J.R. also reports honoraria, speaker fees, or advisory roles for GSK, Takeda, Gilead, Cynata, Pfizer, Spark, Novartis, Celgene, Bluebird Bio, Shire, Avrobio, ATARA, and Bayer; stocks in Genea; and a consultant role for Rarecyte (stocks in lieu).
Figures
References
-
- Siegel R.L., Miller K.D., Fuchs H.E., Jemal A. Cancer statistics, 2021. CA Cancer J. Clin. 2021;71:7–33. - PubMed
-
- Rahib L., Smith B.D., Aizenberg R., Rosenzweig A.B., Fleshman J.M., Matrisian L.M. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. - PubMed
-
- Masiak-Segit W., Rawicz-Pruszynski K., Skorzewska M., Polkowski W.P. Surgical treatment of pancreatic cancer. Pol. Przegl. Chir. 2018;90:45–53. - PubMed
-
- Loveday B., Lipton L., Thomson B. Pancreatic cancer: an update on diagnosis and management. Aust. J. Gen. Pract. 2019;48:826–831. - PubMed
-
- Landman A., Feetham L., Stuckey D. Working together to reduce the burden of pancreatic cancer. Lancet Oncol. 2020;21:334–335. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
