

Associations of Dietary Intakes of Calcium, Magnesium, and Soy Isoflavones With Bone Fracture Risk in Men: A Prospective Study
- PMID: 35229059
- PMCID: PMC8861979
- DOI: 10.1002/jbm4.10563
Associations of Dietary Intakes of Calcium, Magnesium, and Soy Isoflavones With Bone Fracture Risk in Men: A Prospective Study
Abstract
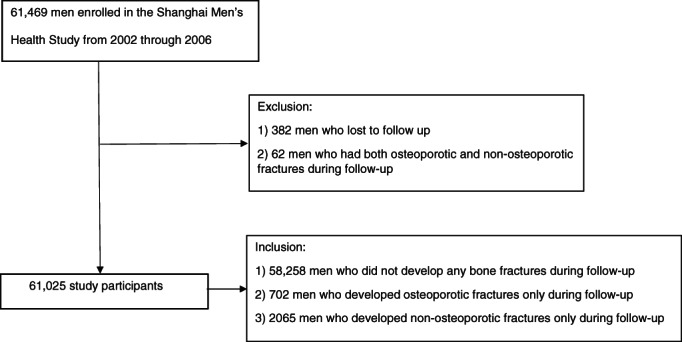
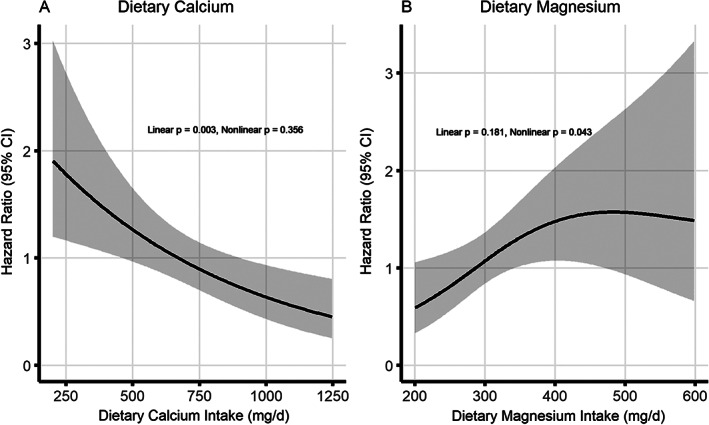
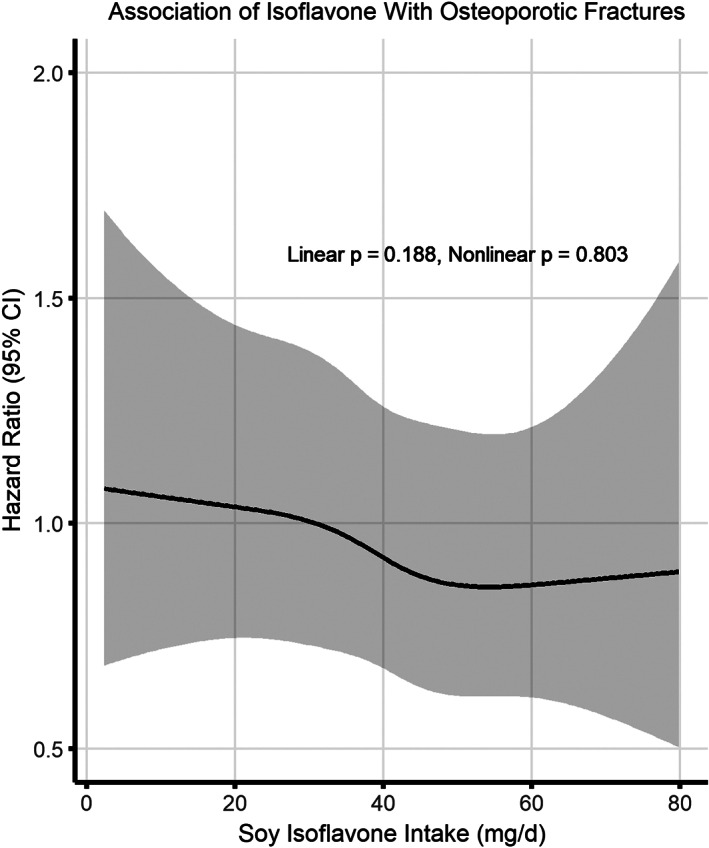
The role of dietary factors in osteoporotic fractures in men is underinvestigated. We examined the associations of dietary intakes of calcium, magnesium, and soy isoflavones with risk of osteoporotic fractures in the Shanghai Men's Health Study. Included in this prospective study were 61,025 men aged 40 to 74 years at study enrollment (2002-2006). The cohort was followed up via in-person surveys for occurrence of bone fractures, major diseases, and survival status. Multivariable Cox regression was applied to evaluate the associations of variables under study (ie, dietary intakes of calcium, magnesium, and soy isoflavones) with incidence of osteoporotic and non-osteoporotic fractures, measured by hazard ratio (HR) and 95% confidence interval (CI). During a median follow-up of 9.5 years, 1.2% and 3.4% of participants experienced osteoporotic or non-osteoporotic fractures, respectively. Dietary calcium intake was inversely associated with risk of osteoporotic fractures with adjusted HRs of 0.78 (95% CI 0.60-1.02) and 0.27 (95% CI 0.13-0.56), respectively, for intake levels of 401 mg/d and >1000 mg/d versus ≤400 mg/d. Higher magnesium intake was associated with increased risk of osteoporotic fractures after adjusting for dietary calcium intake, with HRs of 1.27 (95% CI 0.97-1.66) and 2.21 (95% CI 1.08-4.50), respectively, for intakes of 251 mg/d and >450 mg/d versus intake ≤250 mg/d. High soy isoflavone intake was associated with a 25% reduction of osteoporotic fracture risk (HR = 0.73, 95% CI 0.56-0.97 for soy isoflavone intake >45.2 mg/d versus <21.7 mg/d). Dietary intakes of calcium, magnesium, or soy isoflavones were unrelated to the risk of non-osteoporotic fractures. Our study added to the evidence that dietary calcium intake was inversely associated with a reduced risk of osteoporotic fractures in a dose-response fashion, while high magnesium intake was associated with an increased risk. Our study also revealed a novel association between higher soy isoflavone consumption and osteoporotic fractures in men. © 2021 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Keywords: FRACTURE RISK AND PREVENTION; INTAKES OF CALCIUM AND MAGNESIUM; OSTEOPOROSIS; POPULATION‐BASED PROSPECTIVE STUDY; SOY ISOFLAVONES.
© 2021 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Figures
Similar articles
-
Associations of dietary intakes of calcium, magnesium and soy isoflavones with osteoporotic fracture risk in postmenopausal women: a prospective study.J Nutr Sci. 2022 Aug 1;11:e62. doi: 10.1017/jns.2022.52. eCollection 2022. J Nutr Sci. 2022. PMID: 35992572 Free PMC article.
-
Dietary magnesium and potassium intakes and circulating magnesium are associated with heel bone ultrasound attenuation and osteoporotic fracture risk in the EPIC-Norfolk cohort study.Am J Clin Nutr. 2015 Aug;102(2):376-84. doi: 10.3945/ajcn.114.102723. Epub 2015 Jul 1. Am J Clin Nutr. 2015. PMID: 26135346
-
Soy Food Consumption, Exercise, and Body Mass Index and Osteoporotic Fracture Risk Among Breast Cancer Survivors: The Shanghai Breast Cancer Survival Study.JNCI Cancer Spectr. 2019 Jun;3(2):pkz017. doi: 10.1093/jncics/pkz017. Epub 2019 May 21. JNCI Cancer Spectr. 2019. PMID: 31157323 Free PMC article.
-
Soy, Soy Isoflavones, and Protein Intake in Relation to Mortality from All Causes, Cancers, and Cardiovascular Diseases: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies.J Acad Nutr Diet. 2019 Sep;119(9):1483-1500.e17. doi: 10.1016/j.jand.2019.04.011. Epub 2019 Jul 2. J Acad Nutr Diet. 2019. PMID: 31278047
-
Association between Dietary Isoflavones in Soy and Legumes and Endometrial Cancer: A Systematic Review and Meta-Analysis.J Acad Nutr Diet. 2018 Apr;118(4):637-651. doi: 10.1016/j.jand.2016.09.036. Epub 2016 Dec 1. J Acad Nutr Diet. 2018. PMID: 27914914
Cited by
-
Inquiry of the Metabolic Traits in Relationship with Daily Magnesium Intake: Focus on Type 2 Diabetic Population.Clin Pract. 2024 Jul 8;14(4):1319-1347. doi: 10.3390/clinpract14040107. Clin Pract. 2024. PMID: 39051301 Free PMC article. Review.
-
Assessment of Awareness and Knowledge about Osteoporosis in Relation to Health Prevention among Patients Treated in Osteoporosis Clinics.J Clin Med. 2023 Sep 24;12(19):6157. doi: 10.3390/jcm12196157. J Clin Med. 2023. PMID: 37834801 Free PMC article.
-
Effects of Isoflavonoid and Vitamin D Synergism on Bone Mineral Density-A Systematic and Critical Review.Nutrients. 2023 Dec 5;15(24):5014. doi: 10.3390/nu15245014. Nutrients. 2023. PMID: 38140273 Free PMC article. Review.
-
The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials.Antioxidants (Basel). 2023 Oct 5;12(10):1830. doi: 10.3390/antiox12101830. Antioxidants (Basel). 2023. PMID: 37891909 Free PMC article. Review.
-
The health effects of soy: A reference guide for health professionals.Front Nutr. 2022 Aug 11;9:970364. doi: 10.3389/fnut.2022.970364. eCollection 2022. Front Nutr. 2022. PMID: 36034914 Free PMC article. Review.
References
-
- Office of the Surgeon General (US) . Bone health and osteoporosis: a report of the surgeon general. Rockville, MD: Office of the Surgeon General (US); 2004. - PubMed
-
- Burge R, Dawson‐Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis‐related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465‐475. - PubMed
-
- Lewis JR, Voortman T, Ioannidis JPA. Evaluating and strengthen the evidence for nutritional bone research: ready to break new ground? J Bone Miner Res. 2021;36:219‐226. - PubMed
-
- Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists/American College of Endocrinology: clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2020 update. Endocr Pract. 2020;26(Suppl 1):1‐46. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials