

Multiparametric MRI evaluation of bone sarcomas in children
- PMID: 35229206
- PMCID: PMC8885969
- DOI: 10.1186/s13244-022-01177-9
Multiparametric MRI evaluation of bone sarcomas in children
Abstract
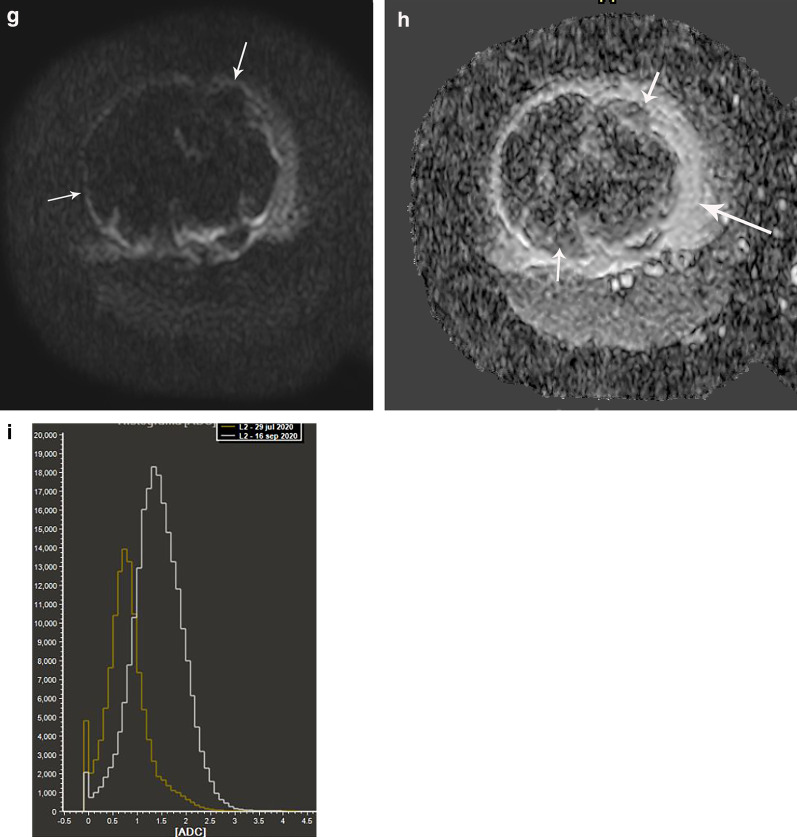
Osteosarcoma and Ewing sarcoma are the most common bone sarcomas in children. Their clinical presentation is very variable depending on the age of the patient and tumor location. MRI is the modality of choice to assess these bone sarcomas and has an important function at diagnosis and also for monitoring recurrence or tumor response. Anatomic sequences include T1- and T2-weighted images and provide morphological assessment that is crucial to localize the tumor and describe anatomical boundaries. Multiparametric MRI provides functional information that helps in the assessment of tumor response to therapy by using different imaging sequences and biomarkers. This review manuscript illustrates the role of MRI in osteosarcoma and Ewing sarcoma in the pediatric population, with emphasis on a functional perspective, highlighting the use of diffusion-weighted imaging and dynamic contrast-enhanced MRI at diagnosis, and during and after treatment.
Keywords: Ewing sarcoma; MRI; Osteosarcoma; Pediatric.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures









References
-
- WHO Classification of Tumours Editorial Board . Soft tissue and bone tumours. Lyon, France: International Agency for Research on Cancer Press; 2020.
-
- Wang CS, Yin QH, Liao JS, et al. Primary diaphyseal osteosarcoma in long bones: imaging features and tumor characteristics. Eur J Radiol. 2012;81:3397–3403. - PubMed
-
- Alsharief AN, Martinez-Rios C, Hopyan S, Amirabadi A, Doria AS, Greer MLC. Usefulness of diffusion-weighted MRI in the initial assessment of osseous sarcomas in children and adolescents. Pediatr Radiol. 2019;49:1201–1208. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
