

Melasma: The need for tailored photoprotection to improve clinical outcomes
- PMID: 35229368
- PMCID: PMC9790748
- DOI: 10.1111/phpp.12783
Melasma: The need for tailored photoprotection to improve clinical outcomes
Abstract
Background/purpose: Melasma is a frequent photoexacerbated hyperpigmentary disorder, which can significantly impact on the quality of life. We sought to review the pathogenesis of melasma, and the role of photoprotection in the prevention and treatment of this disorder.
Methods: We conducted a narrative review of the literature. We performed literature searches with PubMed from January 1990 to December 2021 using the keywords "melasma," "pathogenesis," "ultraviolet radiation," "visible light," "photoprotection," and "sunscreens."
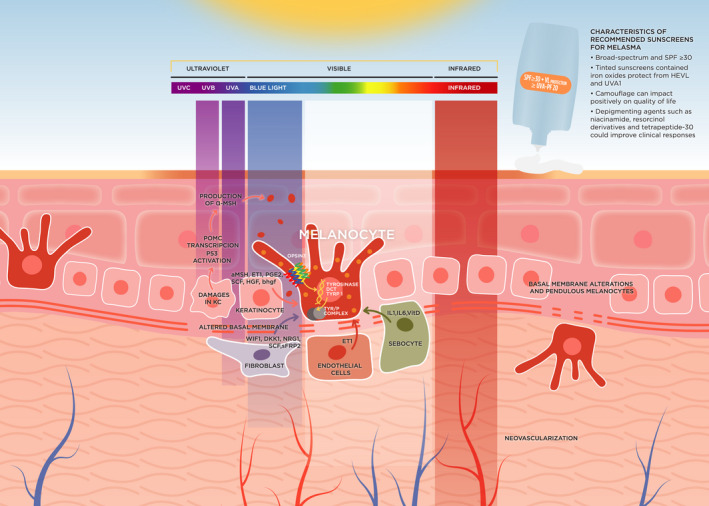
Results: The physiopathology of melasma includes a complex interaction between genetics, sex hormones, and sun exposure. Visible light, in particular high-energy visible light (HEVL), and long-wave UVA (UVA1) play a key role in melasma pathophysiology, and recent research suggests that melasma shares many features with photoaging disorders. Melasma disproportionately affects dark-skinned individuals. Some 30% to 50% of South Americans and Asians, among other ethnicities, can present with melasma. Dark-skinned patients take fewer photoprotective measures. Also, the majority of melasma patients do not adequately follow photoprotection recommendations, including the application of sunscreen. Intensive use of a broad-spectrum sunscreen can prevent melasma in high-risk individuals, can lessen melasma severity (associated or not with depigmenting agents), and can reduce relapses.
Conclusions: Due to the physiopathology of melasma, sunscreens should be broad-spectrum with high sun protection factor, and provide high protection against UVA1 and VL. Sunscreens should be cosmetically acceptable and leave no white residue. Tinted sunscreens are an excellent choice, as pigments can protect from HEVL and UVA1, and may provide camouflage, but they must offer colors that match the skin tone of each patient.
Keywords: dark skin; ethnic skin; melasma; photoprotection; skin of color; sunscreens.
© 2022 The Authors. Photodermatology, Photoimmunology & Photomedicine published by John Wiley & Sons Ltd.
Conflict of interest statement
DMC, JPC, and TP have received consultancy fees from ISDIN laboratories. CG, CT are ISDIN employees.
Figures
References
-
- Artzi O, Horovitz T, Bar‐Ilan E, et al. The pathogenesis of melasma and implications for treatment. J Cosmet Dermatol. 2021;20:3432‐3445. - PubMed
-
- Passeron T, Picardo M. Melasma, a photoaging disorder. Pigment Cell Melanoma Res. 2018;31:461‐465. - PubMed
-
- Ortonne JP, Arellano I, Berneburg M, et al. A global survey of the role of ultraviolet radiation and hormonal influences in the development of melasma. J Eur Acad Dermatol Venereol JEADV. 2009;23:1254‐1262. - PubMed
-
- Hourblin V, Nouveau S, Roy N, de Lacharrière O. Skin complexion and pigmentary disorders in facial skin of 1204 women in 4 Indian cities. Indian J Dermatol Venereol Leprol. 2014;80:395‐401. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
