

Chelation Therapy in Patients With Cardiovascular Disease: A Systematic Review
- PMID: 35229619
- PMCID: PMC9075296
- DOI: 10.1161/JAHA.121.024648
Chelation Therapy in Patients With Cardiovascular Disease: A Systematic Review
Abstract
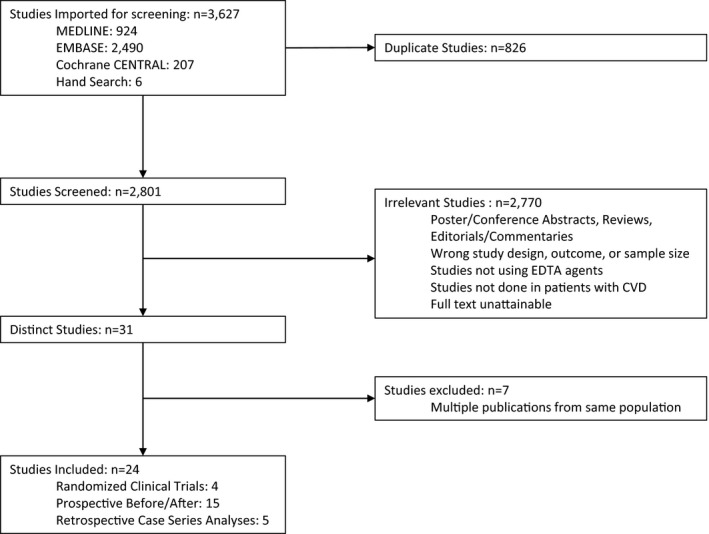
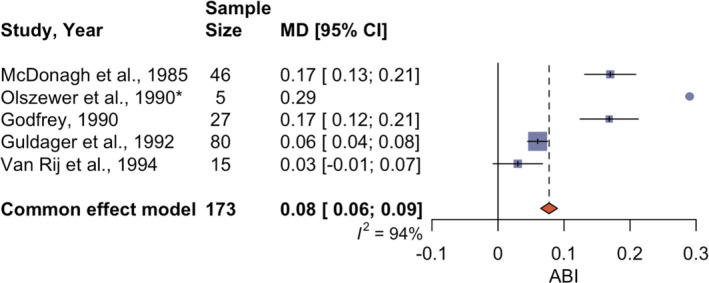
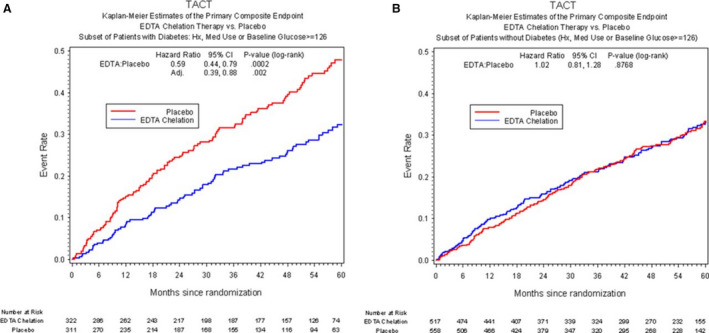
Background EDTA is an intravenous chelating agent with high affinity to divalent cations (lead, cadmium, and calcium) that may be beneficial in the treatment of cardiovascular disease (CVD). Although a large randomized clinical trial showed benefit, smaller studies were inconsistent. We conducted a systematic review of published studies to examine the effect of repeated EDTA on clinical outcomes in adults with CVD. Methods and Results We searched 3 databases (MEDLINE, Embase, and Cochrane) from database inception to October 2021 to identify all studies involving EDTA treatment in patients with CVD. Predetermined outcomes included mortality, disease severity, plasma biomarkers of disease chronicity, and quality of life. Twenty-four studies (4 randomized clinical trials, 15 prospective before/after studies, and 5 retrospective case series) assessed the use of repeated EDTA chelation treatment in patients with preexistent CVD. Of these, 17 studies (1 randomized clinical trial) found improvement in their respective outcomes following EDTA treatment. The largest improvements were observed in studies with high prevalence of participants with diabetes and/or severe occlusive arterial disease. A meta-analysis conducted with 4 studies reporting ankle-brachial index indicated an improvement of 0.08 (95% CI, 0.06-0.09) from baseline. Conclusions Overall, 17 studies suggested improved outcomes, 5 reported no statistically significant effect of treatment, and 2 reported no qualitative benefit. Repeated EDTA for CVD treatment may provide more benefit to patients with diabetes and severe peripheral arterial disease. Differences across infusion regimens, including dosage, solution components, and number of infusions, limit comparisons across studies. Additional research is necessary to confirm these findings and to evaluate the potential mediating role of metals. Registration URL: https://www.crd.york.ac.uk/; Unique identifier: CRD42020166505.
Keywords: EDTA; cardiovascular disease; diabetes; systematic review.
Figures

References
-
- Casdorph HR, Farr CH. EDTA chelation therapy III: treatment of peripheral arterial occlusion, an alternative to amputation. J Holist Med. 1983;5:3–15.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
