

Association Between Inappropriately Dosed Anticoagulation Therapy With Stroke Severity and Outcomes in Patients With Atrial Fibrillation
- PMID: 35229642
- PMCID: PMC9075280
- DOI: 10.1161/JAHA.121.024402
Association Between Inappropriately Dosed Anticoagulation Therapy With Stroke Severity and Outcomes in Patients With Atrial Fibrillation
Abstract
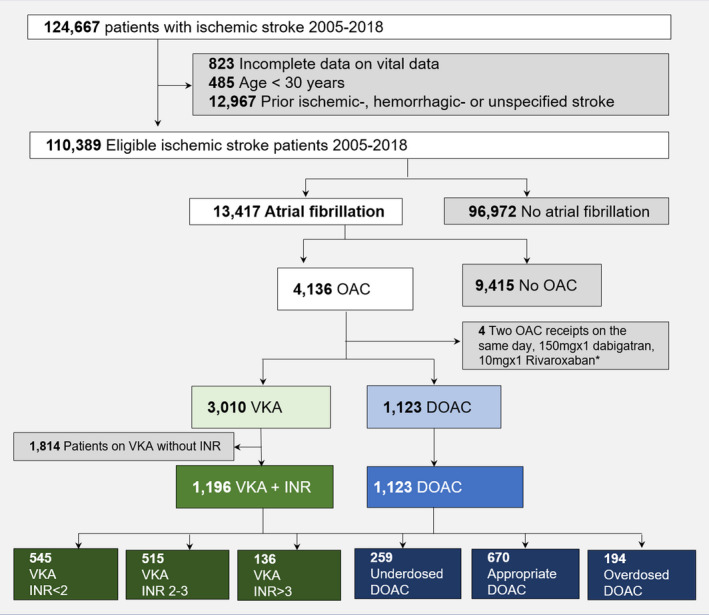
Background Oral anticoagulation (OAC) is effective for stroke prevention in patients with atrial fibrillation. However, some patients experience stroke despite OAC therapy, and knowledge about the impact of prior treatment quality is lacking. Methods and Results Patients with atrial fibrillation on OAC therapy who had a first-time ischemic stroke were identified in the Danish Stroke Registry (2005-2018). Patients treated with vitamin K antagonist (VKA) therapy were compared according to the international normalized ratio just before stroke (international normalized ratio <2 [subtherapeutic], international normalized ratio 2-3 [therapeutic], international normalized ratio >3 [supratherapeutic]), and patients on underdosed, appropriately dosed, and overdosed direct OAC (DOAC) therapy were compared. Stroke severity was determined using the Scandinavia Stroke Scale (0-58 points), and the risk of very severe stroke (0-14 points) was analyzed by multivariable logistic regression. One-year mortality was determined using multivariable Cox regression. A total of 2319 patients with atrial fibrillation and stroke were included; 1196 were taking a VKA (subtherapeutic [46%], therapeutic [43%], supratherapeutic [11%]), and 1123 were taking DOAC (underdosed [23%], appropriately dosed [60%], and overdosed [17%]). Subtherapeutic and supratherapeutic VKA therapy (compared with therapeutic) and underdosed DOAC therapy (compared with appropriate and underdosed DOAC) patients were older, more often women, and more comorbid. Subtherapeutic VKA therapy was associated with very severe stroke (odds ratio [OR], 2.06 [95% CI, 1.28-3.31]), whereas supratherapeutic VKA therapy was not (OR, 1.24 [95% CI, 0.60-2.57]) compared with therapeutic VKA therapy. Patients on subtherapeutic and supratherapeutic VKA therapy had a higher 1-year mortality (hazard ratio [HR], 1.66 [95% CI, 1.29-2.13]); HR, 1.55 [95% CI, 1.08-2.22], respectively) than those on therapeutic VKA therapy. Treatment with underdosed or overdosed DOAC therapy was not associated with very severe stroke (OR, 1.27 [95% CI, 0.76-2.15]; OR, 0.73 [95% CI, 0.37-1.43], respectively) and was not associated with 1-year mortality (HR, 1.09 [95% CI, 0.83-1.44]; HR, 0.82 [95% CI, 0.57-1.18], respectively) than appropriate DOAC. Conclusions Half of the patients with atrial fibrillation with stroke were on inappropriate OAC therapy. Subtherapeutic VKA was associated with worse stroke severity and higher mortality rate than therapeutic VKA therapy. Neither underdosed nor overdosed DOAC was associated with worse outcomes in adjusted models compared with appropriately dosed DOAC. This study supports DOAC as a first-line therapy over VKA.
Keywords: anticoagulation; atrial fibrillation; epidemiology; inappropriate anticoagulation; ischemic stroke.
Figures



References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström‐Lundqvist C, Boriani G, Castella M, Dan G‐A, Dilaveris PE, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio‐Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612 - DOI - PubMed
-
- Xian Y, O’Brien EC, Liang LI, Xu H, Schwamm LH, Fonarow GC, Bhatt DL, Smith EE, Olson DM, Maisch L, et al. Association of preceding antithrombotic treatment with acute ischemic stroke severity and in‐hospital outcomes among patients with atrial fibrillation. JAMA. 2017;317:1057–1067. doi: 10.1001/jama.2017.1371 - DOI - PubMed
-
- Almutairi AR, Zhou L, Gellad WF, Lee JK, Slack MK, Martin JR, Lo‐Ciganic WH. Effectiveness and safety of non–vitamin K antagonist oral anticoagulants for atrial fibrillation and venous thromboembolism: a systematic review and meta‐analyses. Clin Ther. 2017;39:1456–1478. doi: 10.1016/j.clinthera.2017.05.358 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
