

Treatment Changes, Healthcare Resource Utilization, and Costs Among Patients with Symptomatic Obstructive Hypertrophic Cardiomyopathy: A Claims Database Study
- PMID: 35230625
- PMCID: PMC9135924
- DOI: 10.1007/s40119-022-00257-7
Treatment Changes, Healthcare Resource Utilization, and Costs Among Patients with Symptomatic Obstructive Hypertrophic Cardiomyopathy: A Claims Database Study
Abstract
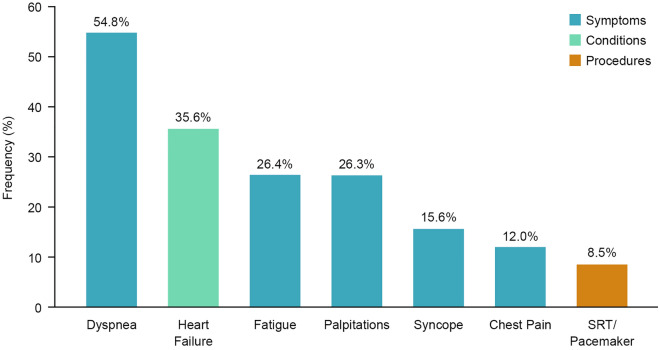
Introduction: There is limited evidence on therapies for obstructive hypertrophic cardiomyopathy (HCM), and data regarding treatment patterns and cost are scarce. This study assessed treatment patterns and economic outcomes in patients with symptomatic obstructive HCM.
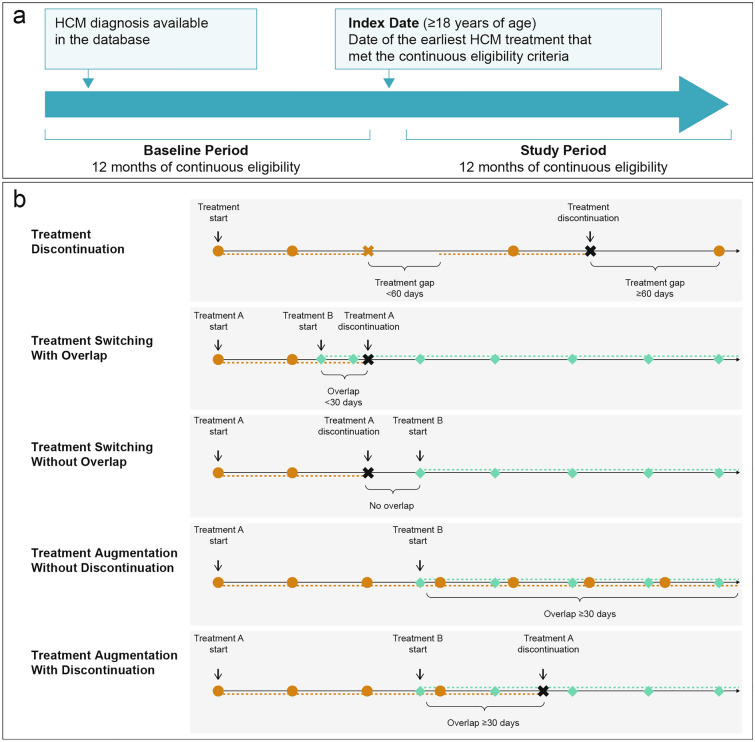
Methods: Adults with symptomatic obstructive HCM as per study design and treated with pharmacotherapies [beta blockers (BBs), calcium channel blockers (CCBs), BB + CCB, or disopyramide] or procedures (septal reduction therapy, heart transplantation, implantable cardioverter-defibrillator, and pacemaker implantation) were identified from the IBM® MarketScan® Commercial and Medicare Supplemental database (January 2009-March 2019). Patients had 12-month continuous eligibility before and after (study period) treatment initiation (index treatment). Healthcare resource utilization (HRU), costs, and treatment changes were assessed.
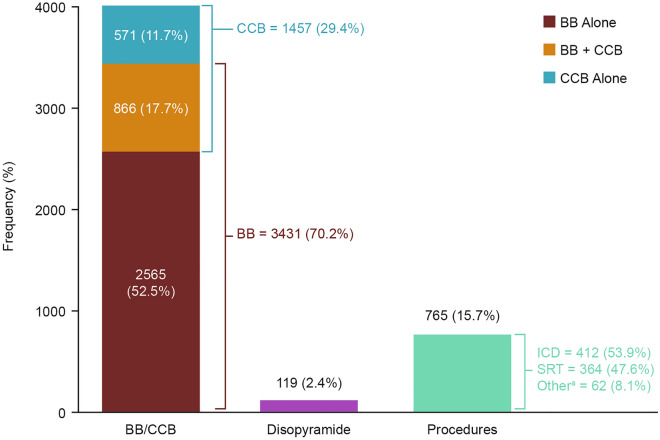
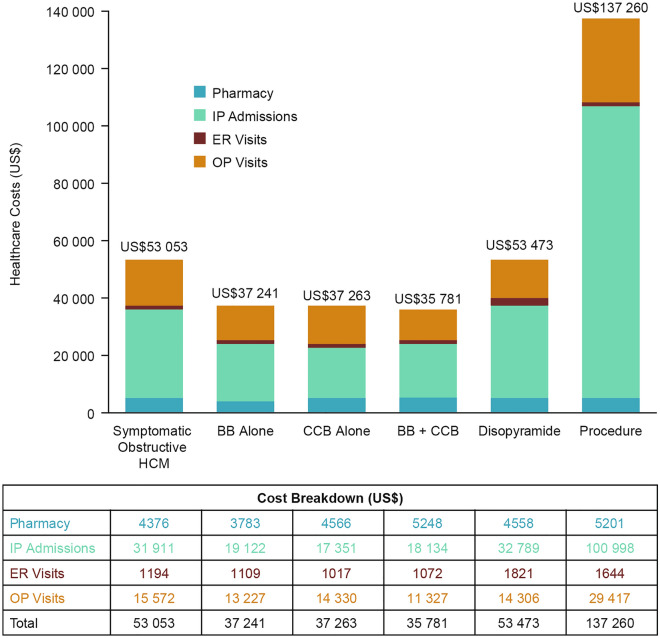
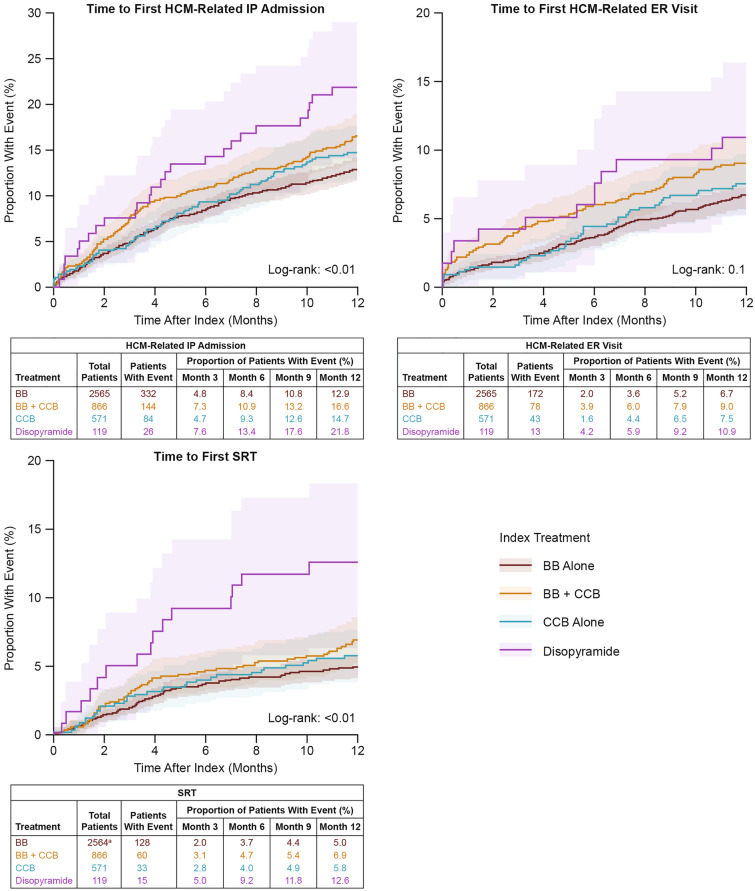
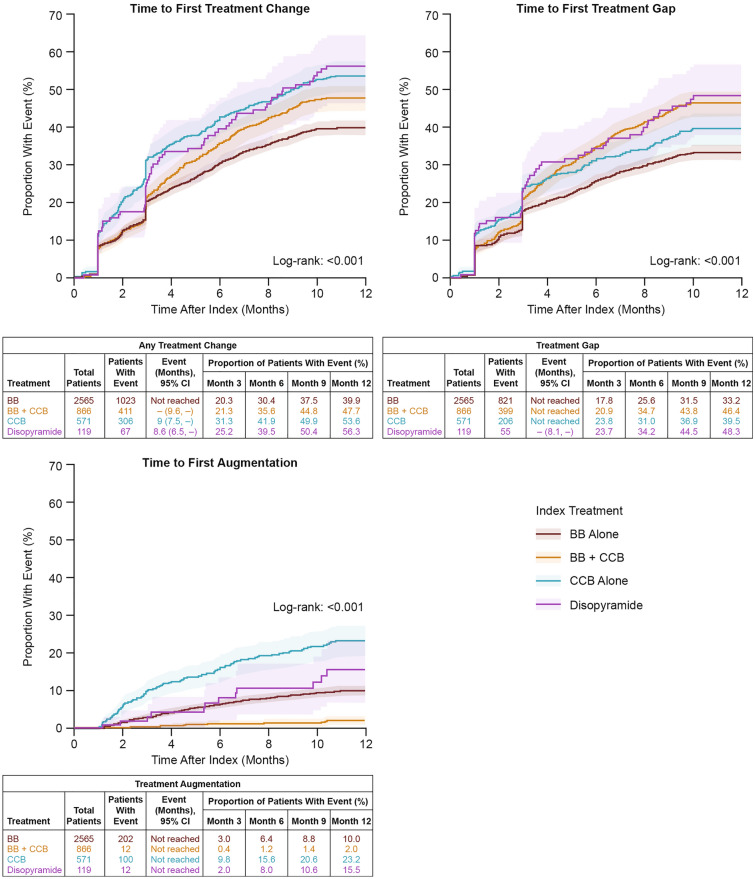
Results: Of the 4883 patients included in the analysis, 85% received pharmacotherapies (BB 52.5%; CCB 11.7%; BB + CCB 17.7%; disopyramide 2.4%) and 15.7% underwent procedures. During the study period, 38, 34, and 100% of all patients had ≥ 1 inpatient stay, emergency room (ER) visit, and outpatient visit, respectively; mean total healthcare costs were US$53,053. Patients undergoing procedures had the highest HRU and costs across groups. Among patients receiving pharmacotherapies, HRU was lowest with BBs and highest with disopyramide. Treatment changes were observed in 43.8% of patients receiving pharmacotherapies.
Conclusions: Patients experienced high rates of treatment changes, and the economic burden associated with symptomatic obstructive HCM increased as therapy escalated. More effective therapies are needed to stabilize or decrease the economic burden of obstructive HCM.
Keywords: Healthcare costs; Healthcare resource utilization; Obstructive hypertrophic cardiomyopathy; Treatment change.
© 2022. The Author(s).
Figures

References
-
- Elliott PM, Anastasakis A, Borger MA, et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC) Eur Heart J. 2014;35:2733–2779. doi: 10.1093/eurheartj/ehu199. - DOI - PubMed
-
- Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2020;76:e159–240. doi: 10.1016/j.jacc.2020.08.045. - DOI - PubMed
-
- Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58:e212–e260. doi: 10.1016/j.jacc.2011.06.011. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
