

Daily prefrontal closed-loop repetitive transcranial magnetic stimulation (rTMS) produces progressive EEG quasi-alpha phase entrainment in depressed adults
- PMID: 35231608
- PMCID: PMC8979612
- DOI: 10.1016/j.brs.2022.02.008
Daily prefrontal closed-loop repetitive transcranial magnetic stimulation (rTMS) produces progressive EEG quasi-alpha phase entrainment in depressed adults
Abstract
Background: Transcranial magnetic stimulation (TMS) is a non-invasive neuromodulation modality that can treat depression, obsessive-compulsive disorder, or help smoking cessation. Research suggests that timing the delivery of TMS relative to an endogenous brain state may affect efficacy and short-term brain dynamics.
Objective: To investigate whether, for a multi-week daily treatment of repetitive TMS (rTMS), there is an effect on brain dynamics that depends on the timing of the TMS relative to individuals' prefrontal EEG quasi-alpha rhythm (between 6 and 13 Hz).
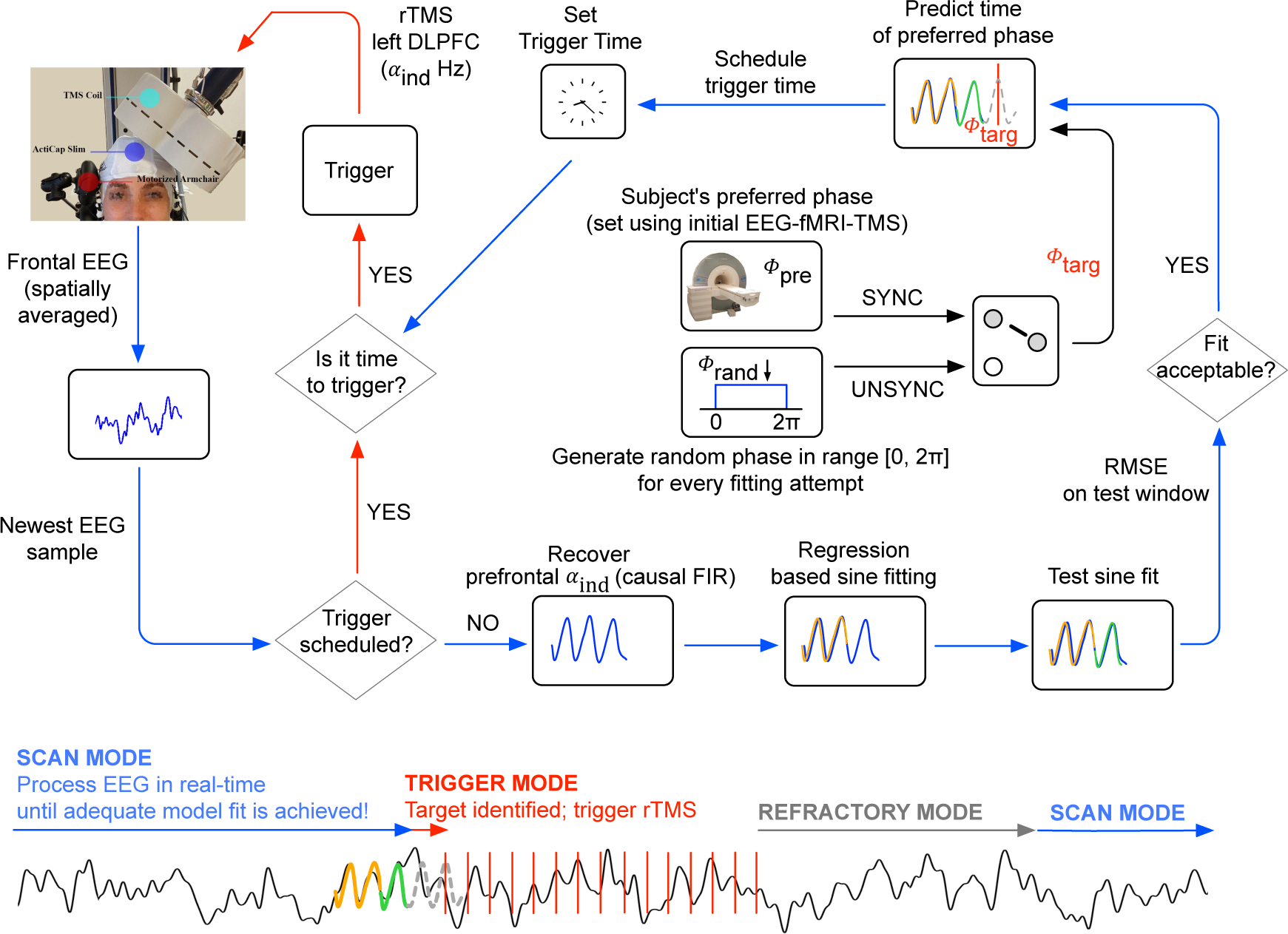
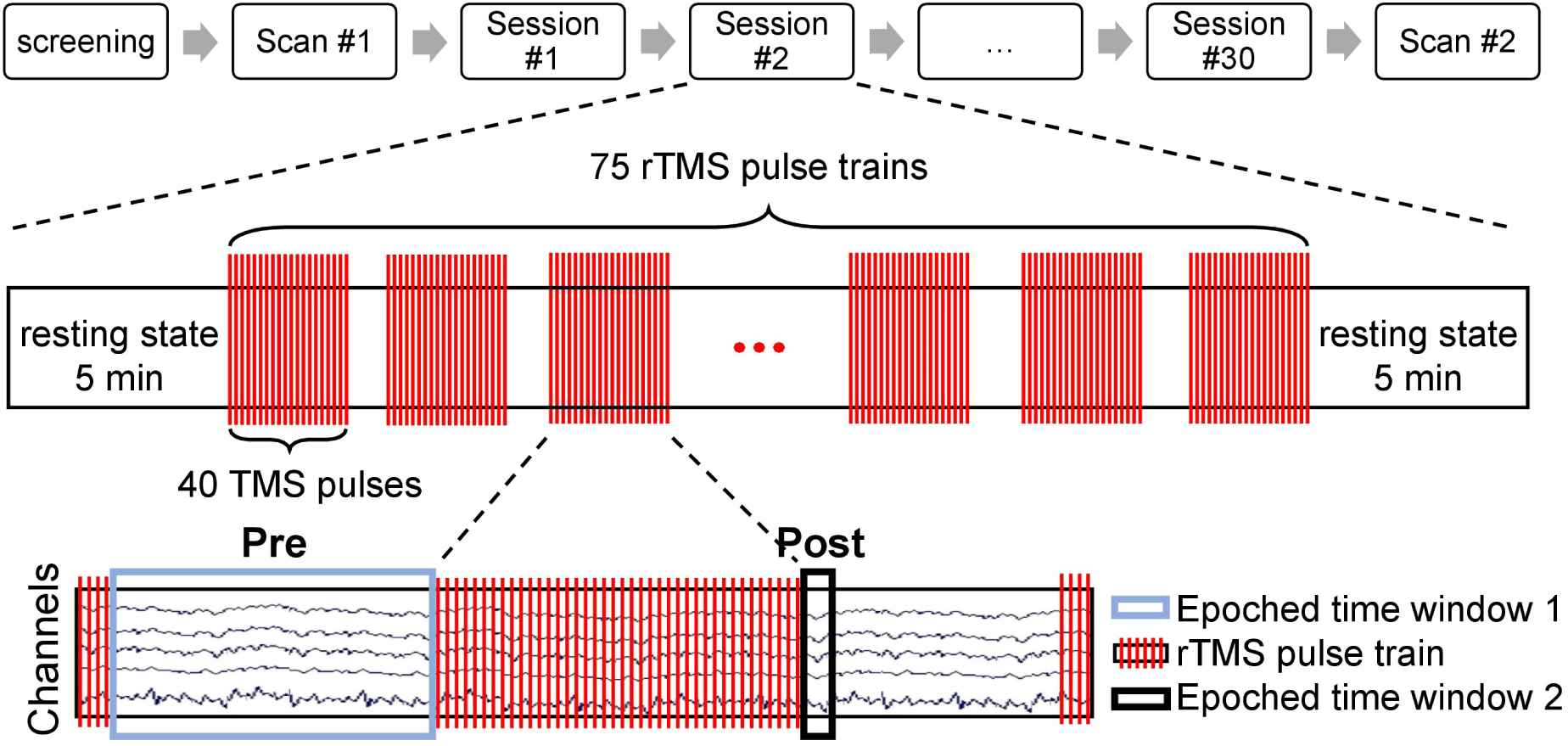
Method: We developed a novel closed-loop system that delivers personalized EEG-triggered rTMS to patients undergoing treatment for major depressive disorder. In a double blind study, patients received daily treatments of rTMS over a period of six weeks and were randomly assigned to either a synchronized or unsynchronized treatment group, where synchronization of rTMS was to their prefrontal EEG quasi-alpha rhythm.
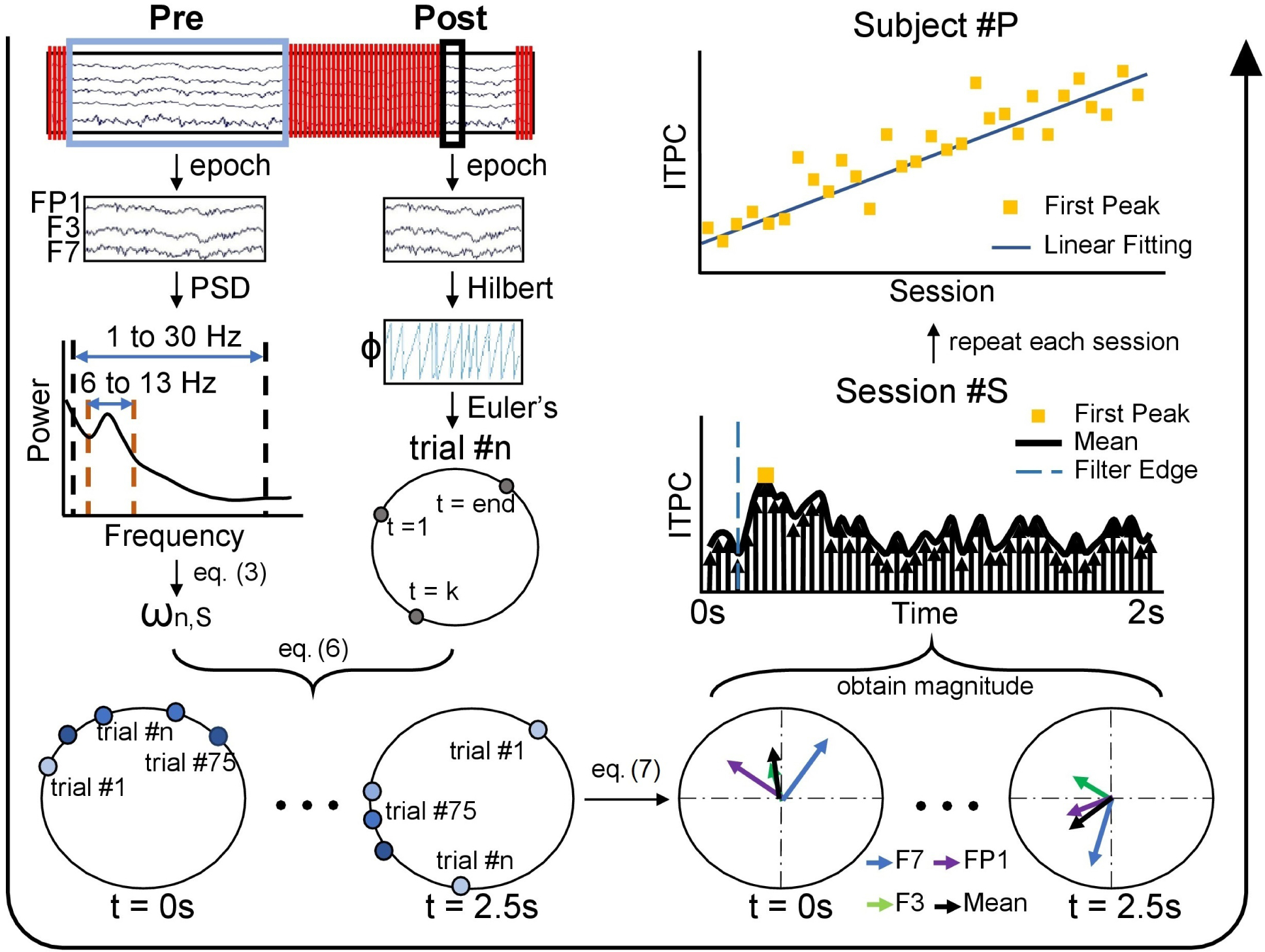
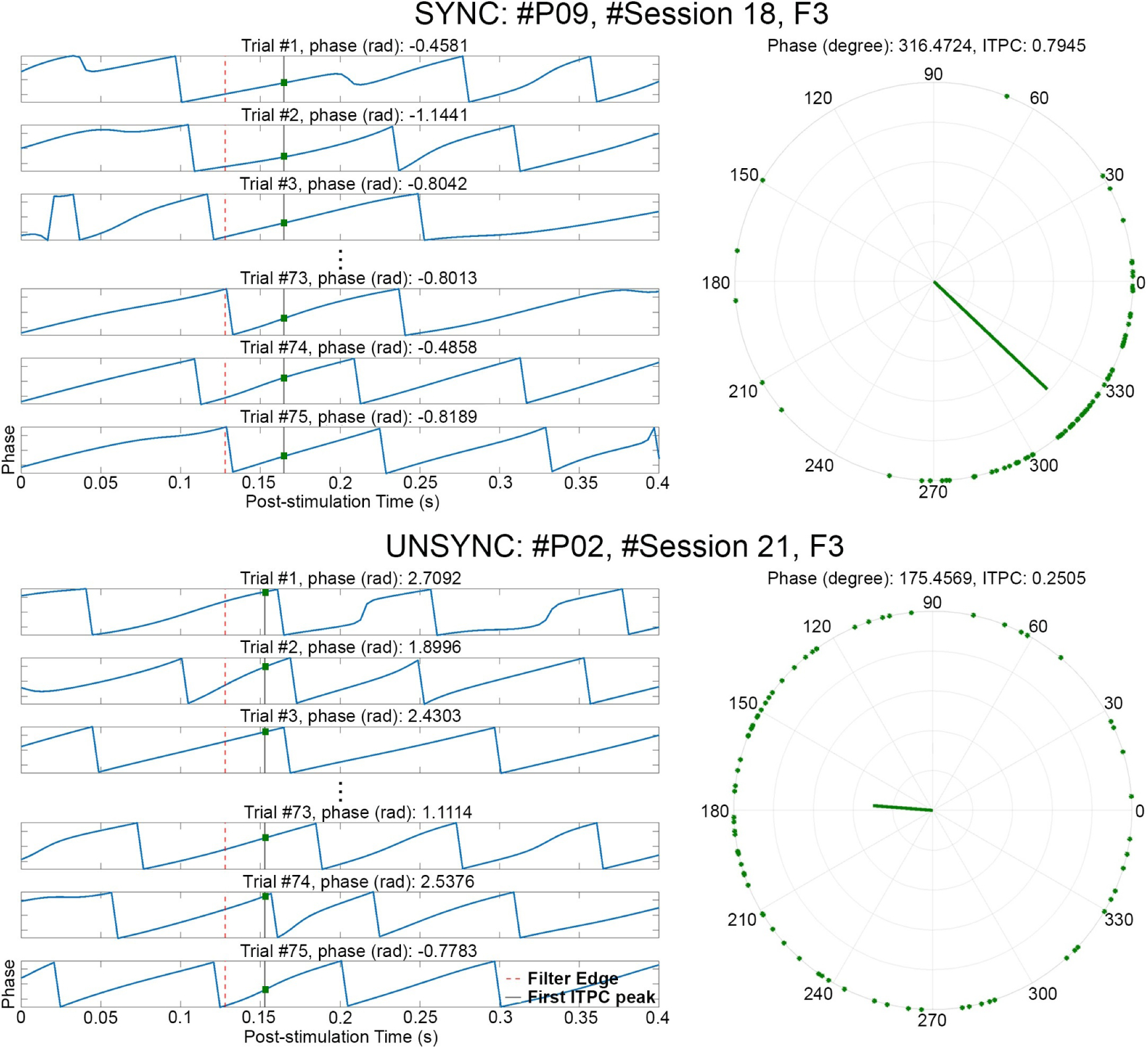
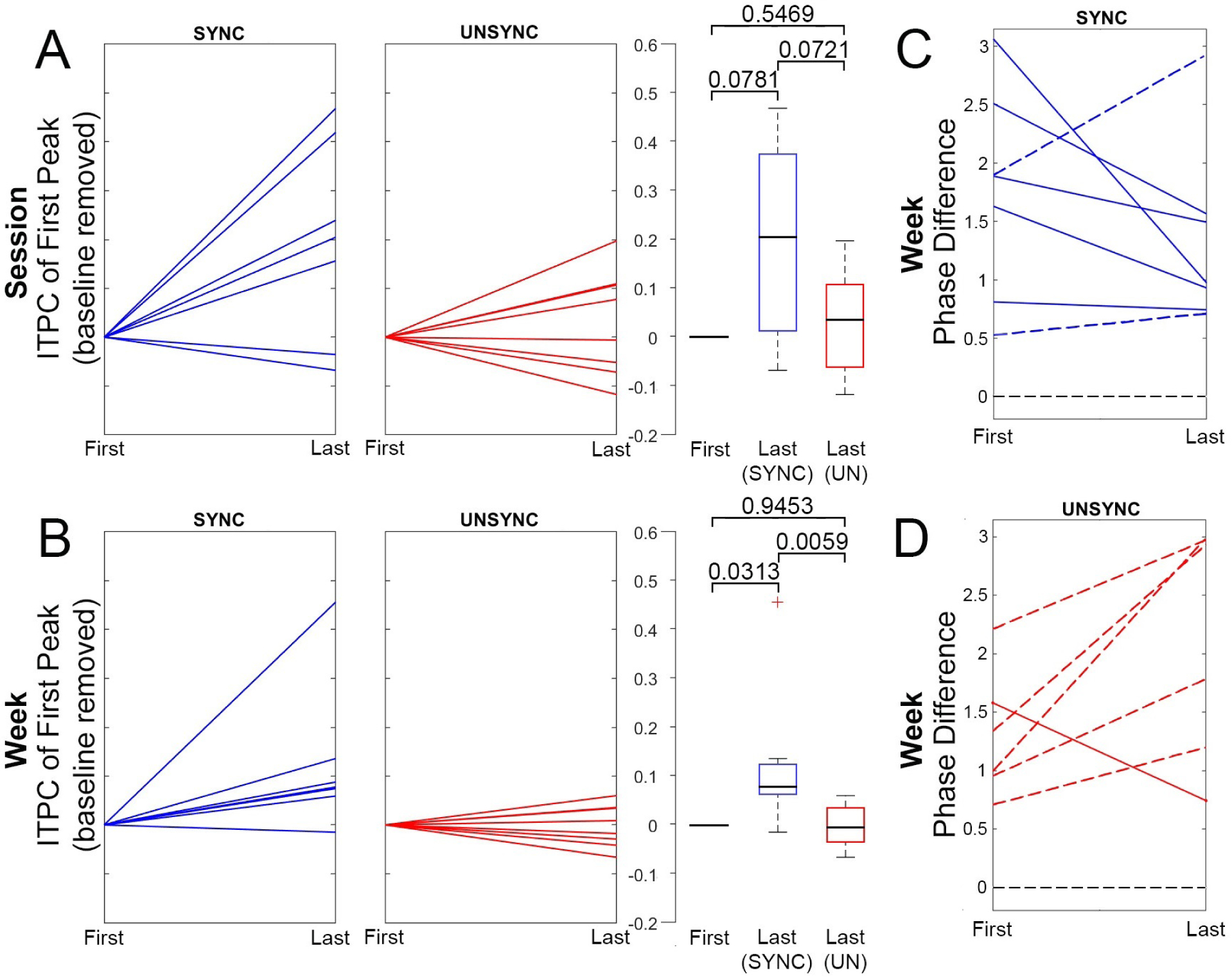
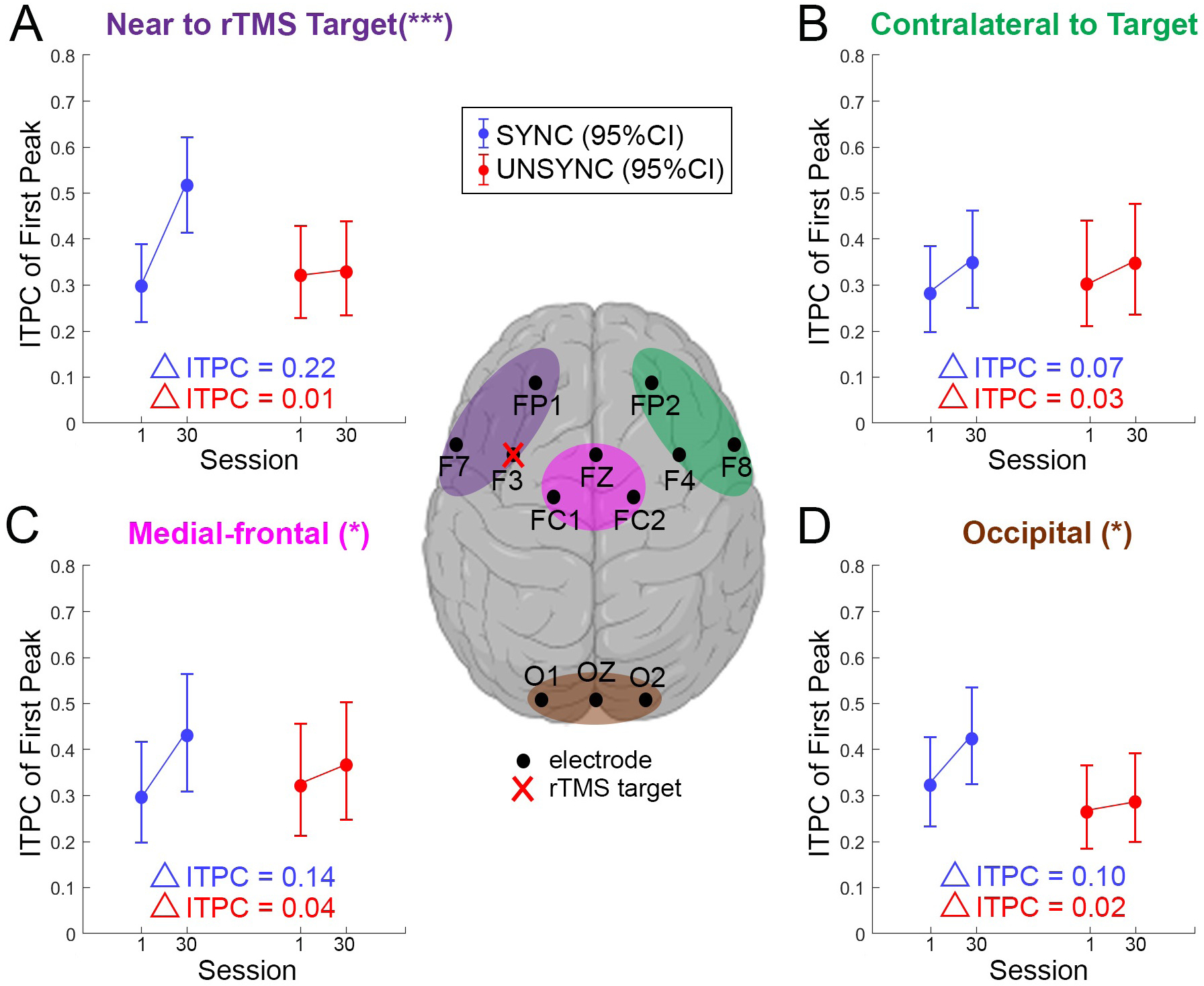
Results: When rTMS is applied over the dorsal lateral prefrontal cortex (DLPFC) and synchronized to the patient's prefrontal quasi-alpha rhythm, patients develop strong phase entrainment over a period of weeks, both over the stimulation site as well as in a subset of areas distal to the stimulation site. In addition, at the end of the course of treatment, this group's entrainment phase shifts to be closer to the phase that optimally engages the distal target, namely the anterior cingulate cortex (ACC). These entrainment effects are not observed in the group that is given rTMS without initial EEG synchronization of each TMS train.
Conclusions: The entrainment effects build over the course of days/weeks, suggesting that these effects engage neuroplastic changes which may have clinical consequences in depression or other diseases.
Keywords: Closed-loop neurostimulation; Electroencephalography (EEG); Inter-trial phase coherence (ITPC); Major depressive disorder (MDD); Repetitive transcranial magnetic stimulation (rTMS).
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
EEG synchronized left prefrontal transcranial magnetic stimulation (TMS) for treatment resistant depression is feasible and produces an entrainment dependent clinical response: A randomized controlled double blind clinical trial.Brain Stimul. 2023 Nov-Dec;16(6):1753-1763. doi: 10.1016/j.brs.2023.11.010. Epub 2023 Dec 2. Brain Stimul. 2023. PMID: 38043646 Free PMC article. Clinical Trial.
-
Brain oscillation-synchronized stimulation of the left dorsolateral prefrontal cortex in depression using real-time EEG-triggered TMS.Brain Stimul. 2020 Jan-Feb;13(1):197-205. doi: 10.1016/j.brs.2019.10.007. Epub 2019 Oct 12. Brain Stimul. 2020. PMID: 31631058 Clinical Trial.
-
The timing of transcranial magnetic stimulation relative to the phase of prefrontal alpha EEG modulates downstream target engagement.Brain Stimul. 2023 May-Jun;16(3):830-839. doi: 10.1016/j.brs.2023.05.007. Epub 2023 May 13. Brain Stimul. 2023. PMID: 37187457
-
[Interactive rTMS protocols in psychiatry].Encephale. 2013 Dec;39(6):426-31. doi: 10.1016/j.encep.2013.04.009. Epub 2013 Jun 28. Encephale. 2013. PMID: 23810752 Review. French.
-
Neuroimaging and neuromodulation approaches to study eating behavior and prevent and treat eating disorders and obesity.Neuroimage Clin. 2015 Mar 24;8:1-31. doi: 10.1016/j.nicl.2015.03.016. eCollection 2015. Neuroimage Clin. 2015. PMID: 26110109 Free PMC article. Review.
Cited by
-
EEG synchronized left prefrontal transcranial magnetic stimulation (TMS) for treatment resistant depression is feasible and produces an entrainment dependent clinical response: A randomized controlled double blind clinical trial.Brain Stimul. 2023 Nov-Dec;16(6):1753-1763. doi: 10.1016/j.brs.2023.11.010. Epub 2023 Dec 2. Brain Stimul. 2023. PMID: 38043646 Free PMC article. Clinical Trial.
-
Modulation of motor excitability reflects traveling waves of neural oscillations.Cell Rep. 2025 Jun 24;44(6):115864. doi: 10.1016/j.celrep.2025.115864. Epub 2025 Jun 14. Cell Rep. 2025. PMID: 40517384 Free PMC article.
-
A randomized controlled trial of alpha phase-locked auditory stimulation to treat symptoms of sleep onset insomnia.Sci Rep. 2024 Jun 6;14(1):13039. doi: 10.1038/s41598-024-63385-1. Sci Rep. 2024. PMID: 38844793 Free PMC article. Clinical Trial.
-
Embracing Internal States: A Review of Optimization of Repetitive Transcranial Magnetic Stimulation for Treating Depression.Neurosci Bull. 2025 May;41(5):866-880. doi: 10.1007/s12264-024-01347-3. Epub 2025 Feb 20. Neurosci Bull. 2025. PMID: 39976854 Review.
-
Real-time TMS-EEG for brain state-controlled research and precision treatment: a narrative review and guide.J Neural Eng. 2024 Nov 1;21(6):061001. doi: 10.1088/1741-2552/ad8a8e. J Neural Eng. 2024. PMID: 39442548 Free PMC article. Review.
References
-
- Akar SA, Kara S, Agambayev S, and Bilgiç V (2015). Nonlinear analysis of EEGs of patients with major depression during different emotional states. Computers in biology and medicine, 67:49–60. - PubMed
-
- Anderson RJ, Hoy KE, Daskalakis ZJ, and Fitzgerald PB (2016). Repetitive transcranial magnetic stimulation for treatment resistant depression: Re-establishing connections. Clinical Neurophysiology, 127(11):3394–3405. - PubMed
-
- Arns M, Cerquera A, Gutiérrez RM, Hasselman F, and Freund JA (2014). Non-linear EEG analyses predict non-response to rTMS treatment in major depressive disorder. Clinical Neurophysiology, 125(7):1392–1399. - PubMed
-
- Bachmann M, Päeske L, Kalev K, Aarma K, Lehtmets A, Ööpik P, Lass J, and Hinrikus H (2018). Methods for classifying depression in single channel EEG using linear and nonlinear signal analysis. Computer methods and programs in biomedicine, 155:11–17. - PubMed
-
- Barbas H, Ghashghaei H, Rempel-Clower N, and Xiao D (2002). Anatomic basis of functional specialization in prefrontal cortices in primates. Handbook of neuropsychology, 7:1–28.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
