

Pulmonary arterial hypertension in hereditary hemorrhagic telangiectasia associated with ACVRL1 mutation: a case report
- PMID: 35232468
- PMCID: PMC8889686
- DOI: 10.1186/s13256-022-03296-9
Pulmonary arterial hypertension in hereditary hemorrhagic telangiectasia associated with ACVRL1 mutation: a case report
Abstract
Introduction: Hereditary hemorrhagic telangiectasia is an autosomal dominant condition with an estimated prevalence of 1 in 5000. It is characterized by the presence of abnormalities of vascular structures, and may affect many organ systems, including the lungs, brain, spinal cord, gastrointestinal tract, and liver. A causative mutation is identified in approximately 97% of patients with definite hereditary hemorrhagic telangiectasia in one of three genes including a mutation in endoglin, a mutation in a locus mapped to chromosome 5, and an activin receptor-like kinase-1 (ACVRL1) mutation that is associated with an increased incidence of primary pulmonary hypertension. Pulmonary arterial hypertension is a rare (15-25 cases per million people) but severe vascular disorder. Heritable pulmonary arterial hypertension is associated with several gene mutations, with 75% having a mutation in the bone morphogenetic protein receptor 2 (BMPR2). However, the remaining 25% of patients have other associated genetic mutations including ACVLR1, which is also associated with hereditary hemorrhagic telangiectasia. Pulmonary arterial hypertension is a rare complication in patients with hereditary hemorrhagic telangiectasia (< 1% of the hereditary hemorrhagic telangiectasia population). We describe a case report with this rare occurrence.
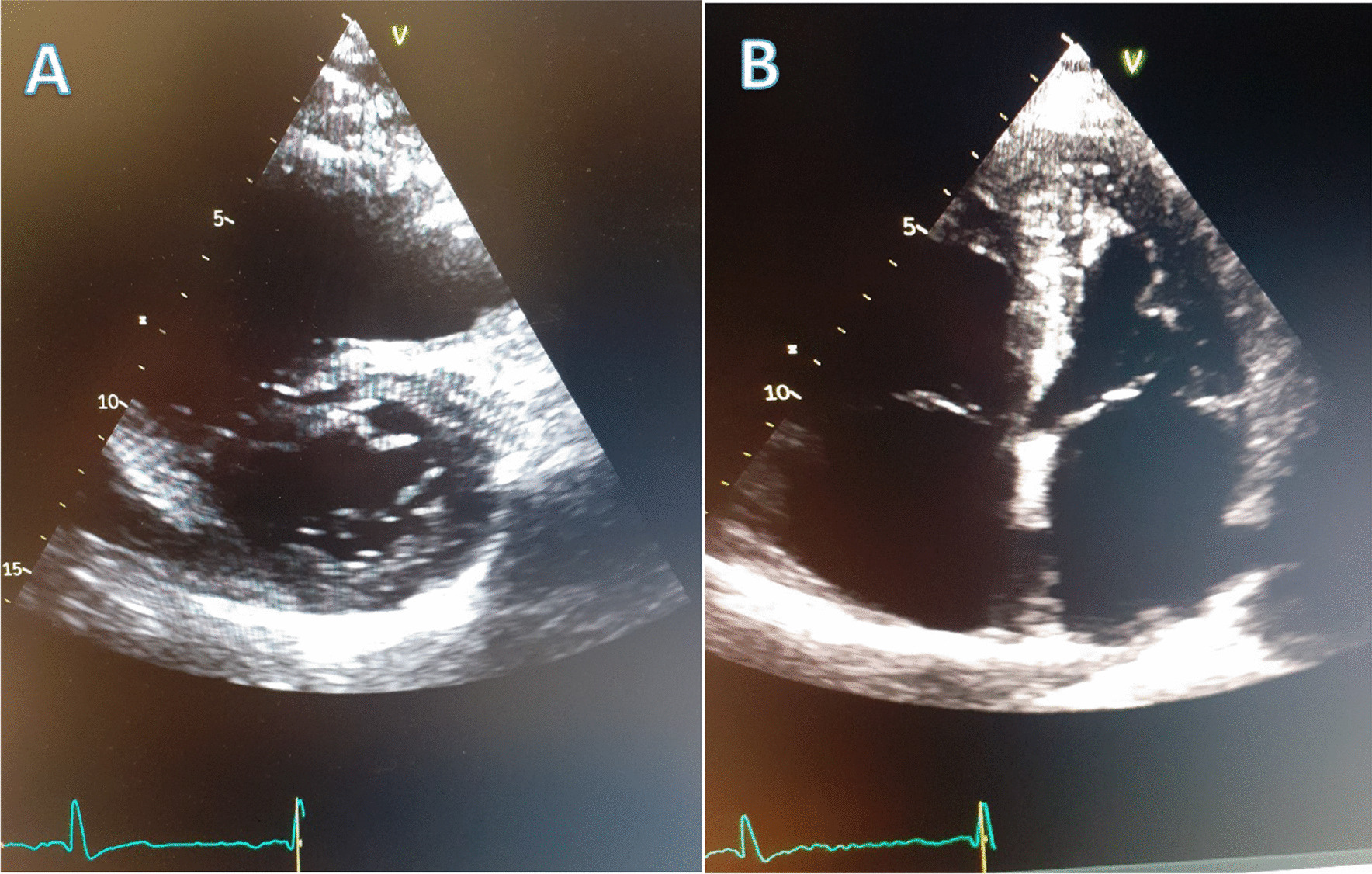
Case presentation: A 70-year-old white/caucasian Irish male presented for screening for hereditary hemorrhagic telangiectasia due to a history of recurrent epistaxis (once/week) and a family history suggestive of pulmonary hypertension. Genetic testing confirmed an ACVRL1 mutation, while an echocardiogram and right heart catheterization confirmed pulmonary arterial hypertension. On examination, he had several mucocutaneous telangiectasia across his face. He was commenced on tadalafil and macitentan. However, this led to increased iron deficiency anemia and pedal edema. Selexipag was also added to his drug regime. He continues to require intermittent admissions for diuresis and blood transfusions.
Conclusion: The association of hereditary hemorrhagic telangiectasia and pulmonary arterial hypertension is rare (< 1%). Here we describe a case of hereditary hemorrhagic telangiectasia complicated with pulmonary arterial hypertension as a result of an ACVRL1 mutation. We also describe the clinical challenges of treating these two conditions together, as treatment options for pulmonary arterial hypertension tend to worsen hereditary hemorrhagic telangiectasia symptoms.
Keywords: Case report; Hereditary hemorrhagic telangiectasia; Pulmonary arterial hypertension.
© 2022. The Author(s).
Conflict of interest statement
There are no competing interests for any of the contributing authors
Figures


References
-
- Faughnan ME, Palda VA, Garcia-Tsao G, Geisthoff UW, McDonald J, Proctor DD, HHT Foundation International—Guidelines Working Group et al. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. 2011;48(2):73–87. doi: 10.1136/jmg.2009.069013. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
