

Survival for waitlisted kidney failure patients receiving transplantation versus remaining on waiting list: systematic review and meta-analysis
- PMID: 35232772
- PMCID: PMC8886447
- DOI: 10.1136/bmj-2021-068769
Survival for waitlisted kidney failure patients receiving transplantation versus remaining on waiting list: systematic review and meta-analysis
Abstract
Objectives: To investigate the survival benefit of transplantation versus dialysis for waitlisted kidney failure patients with a priori stratification.
Design: Systematic review and meta-analysis.
Data sources: Online databases MEDLINE, Ovid Embase, Web of Science, Cochrane Collection, and ClinicalTrials.gov were searched between database inception and 1 March 2021.
Inclusion criteria: All comparative studies that assessed all cause mortality for transplantation versus dialysis in patients with kidney failure waitlisted for transplant surgery were included. Two independent reviewers extracted the data and assessed the risk of bias of included studies. Meta-analysis was done using the DerSimonian-Laird random effects model, with heterogeneity investigated by subgroup analyses, sensitivity analyses, and meta-regression.
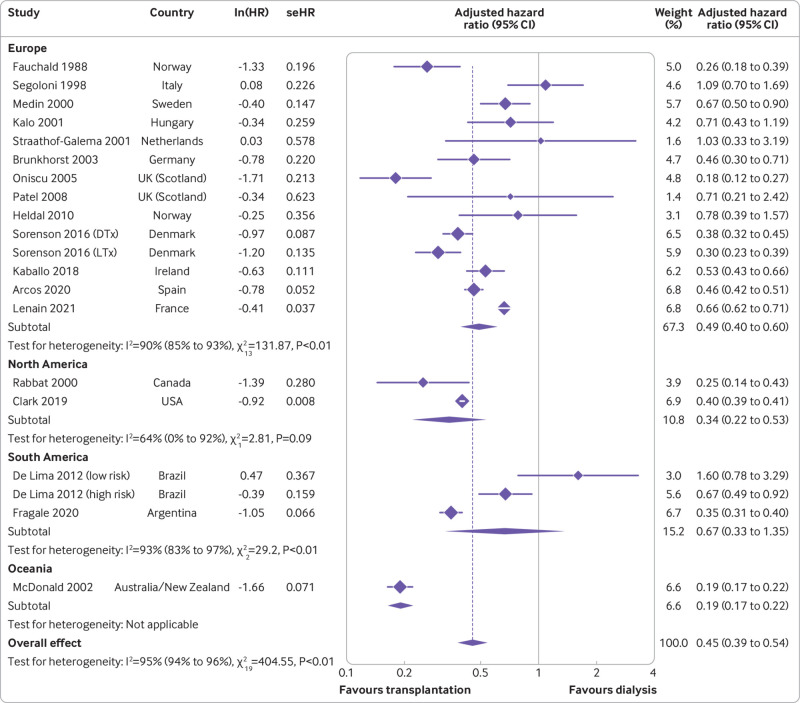
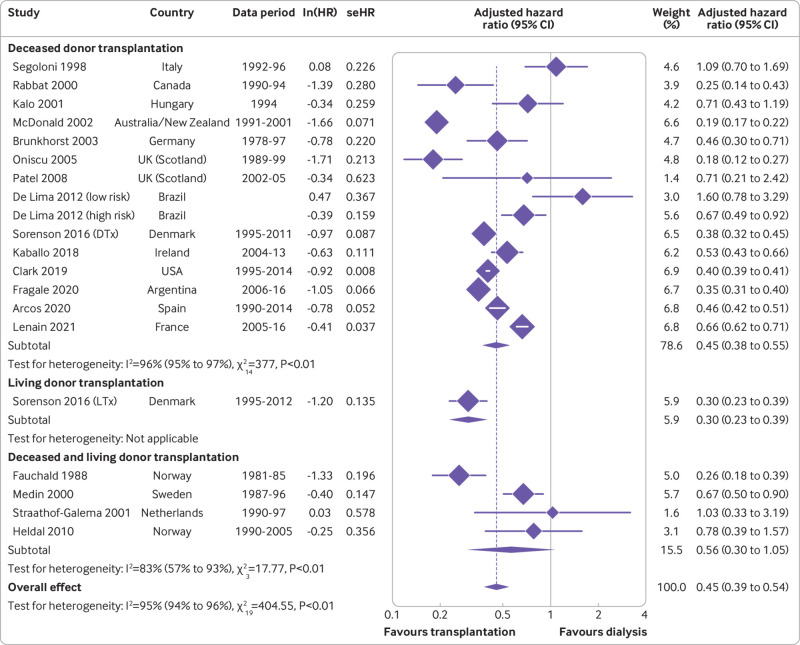
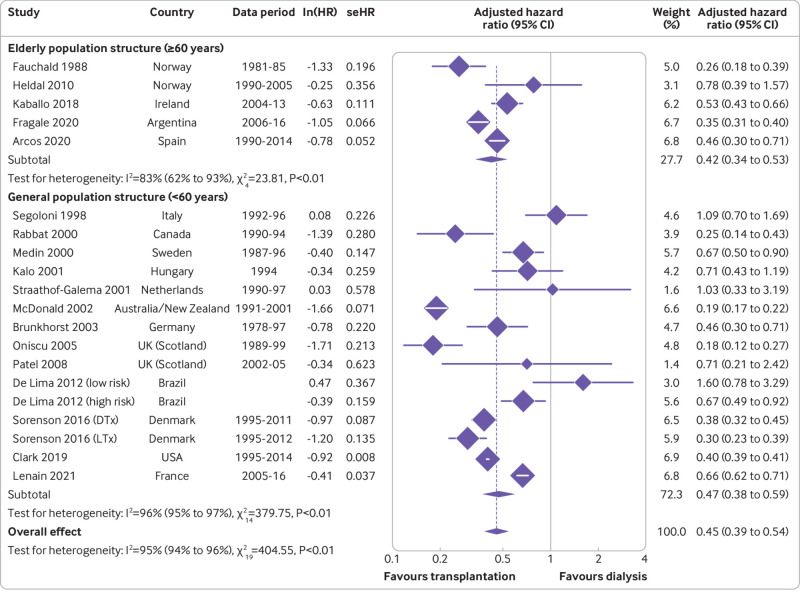
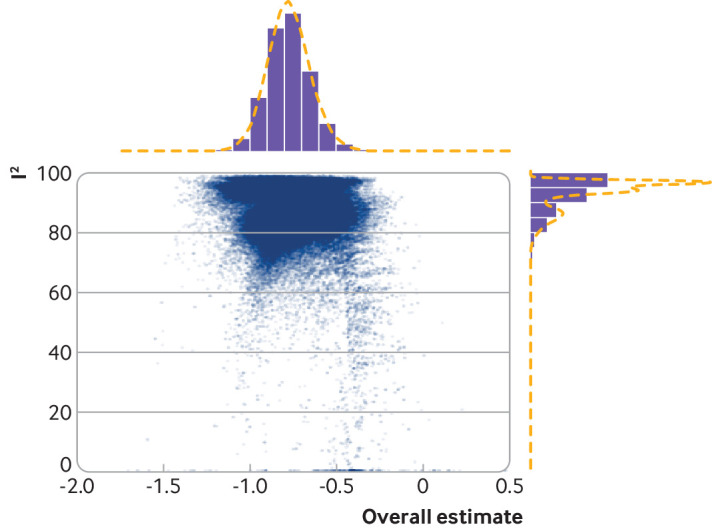
Results: The search identified 48 observational studies with no randomised controlled trials (n=1 245 850 patients). In total, 92% (n=44/48) of studies reported a long term (at least one year) survival benefit associated with transplantation compared with dialysis. However, 11 of those studies identified stratums in which transplantation offered no statistically significant benefit over remaining on dialysis. In 18 studies suitable for meta-analysis, kidney transplantation showed a survival benefit (hazard ratio 0.45, 95% confidence interval 0.39 to 0.54; P<0.001), with significant heterogeneity even after subgroup/sensitivity analyses or meta-regression analysis.
Conclusion: Kidney transplantation remains the superior treatment modality for most patients with kidney failure to reduce all cause mortality, but some subgroups may lack a survival benefit. Given the continued scarcity of donor organs, further evidence is needed to better inform decision making for patients with kidney failure.
Study registration: PROSPERO CRD42021247247.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: DC had support from the Royal College of Surgeons (England) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures

Comment in
-
Counting chronic kidney disease in developing countries.BMJ. 2022 Apr 6;377:o889. doi: 10.1136/bmj.o889. BMJ. 2022. PMID: 35387782 No abstract available.
References
-
- UK Renal Renal Registry. UK Renal Registry 23rd Annual Report: data to 31/12/2019. 2021. renal.org/audit-research/annual-report.
-
- NHS Blood and Transplant. Organ and Tissue Donation and Transplantation: Activity Report 2020/21. 2021. https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/24053/activit....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical