

COVID-19 in pregnancy-what study designs can we use to assess the risk of congenital anomalies in relation to COVID-19 disease, treatment and vaccination?
- PMID: 35234297
- PMCID: PMC9115419
- DOI: 10.1111/ppe.12840
COVID-19 in pregnancy-what study designs can we use to assess the risk of congenital anomalies in relation to COVID-19 disease, treatment and vaccination?
Abstract
Background: The COVID-19 pandemic has accelerated pregnancy outcome research, but little attention has been given specifically to the risk of congenital anomalies (CA) and first trimester exposures.
Objectives: We reviewed the main data sources and study designs used internationally, particularly in Europe, for CA research, and their strengths and limitations for investigating COVID-19 disease, medications and vaccines.
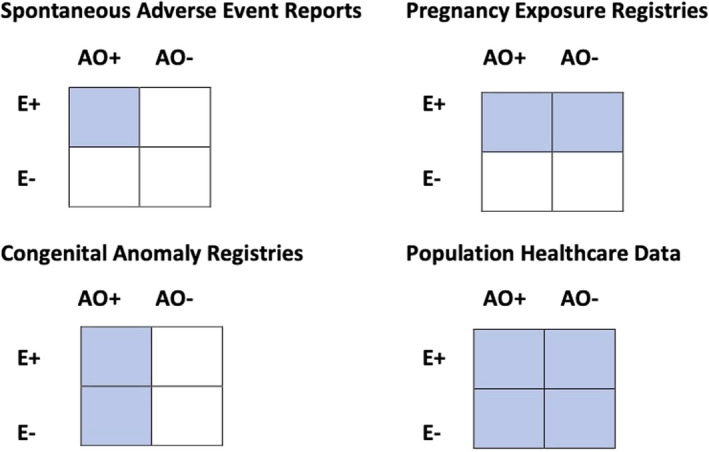
Population: We classify research designs based on four data sources: a) spontaneous adverse event reporting, where study subjects are positive for both exposure and outcome, b) pregnancy exposure registries, where study subjects are positive for exposure, c) congenital anomaly registries, where study subjects are positive for outcome and d) population healthcare data where the entire population of births is included, irrespective of exposure and outcome.
Study design: Each data source allows different study designs, including case series, exposed pregnancy cohorts (with external comparator), ecological studies, case-control studies and population cohort studies (with internal comparator).
Methods: The quality of data sources for CA studies is reviewed in relation to criteria including diagnostic accuracy of CA data, size of study population, inclusion of terminations of pregnancy for foetal anomaly, inclusion of first trimester COVID-19-related exposures and use of an internal comparator group. Multinational collaboration models are reviewed.
Results: Pregnancy exposure registries have been the main design for COVID-19 pregnancy studies, but lack detail regarding first trimester exposures relevant to CA, or a suitable comparator group. CA registries present opportunities for improving diagnostic accuracy in COVID-19 research, especially when linked to other data sources. Availability of inpatient hospital medication use in population healthcare data is limited. More use of ongoing mother-baby linkage systems would improve research efficiency. Multinational collaboration delivers statistical power.
Conclusions: Challenges and opportunities exist to improve research on CA in relation to the COVID-19 pandemic and future pandemics.
Keywords: COVID-19; congenital anomalies; healthcare databases; pregnancy cohorts; registries; study design.
© 2022 The Authors. Paediatric and Perinatal Epidemiology published by John Wiley & Sons Ltd.
Figures
References
-
- Delahoy MJ, Whitaker M, O’Halloran A, Chai SJ, Kirley PD, Alden N, et al. Characteristics and maternal and birth outcomes of hospitalized pregnant women with laboratory‐confirmed COVID‐19 — COVID‐NET, 13 States, March 1–August 22, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1347–1354. doi: 10.15585/mmwr.mm6938e1. - DOI - PMC - PubMed
-
- Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, Kew T, et al. for PregCOV‐19 Living Systematic Review Consortium . Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta‐analysis. BMJ. 2020;1(370):m3320. doi: 10.1136/bmj.m3320. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
