

eDOL mHealth App and Web Platform for Self-monitoring and Medical Follow-up of Patients With Chronic Pain: Observational Feasibility Study
- PMID: 35234654
- PMCID: PMC8928045
- DOI: 10.2196/30052
eDOL mHealth App and Web Platform for Self-monitoring and Medical Follow-up of Patients With Chronic Pain: Observational Feasibility Study
Abstract
Background: Chronic pain affects approximately 30% of the general population, severely degrades quality of life (especially in older adults) and professional life (inability or reduction in the ability to work and loss of employment), and leads to billions in additional health care costs. Moreover, available painkillers are old, with limited efficacy and can cause significant adverse effects. Thus, there is a need for innovation in the management of chronic pain. Better characterization of patients could help to identify the predictors of successful treatments, and thus, guide physicians in the initial choice of treatment and in the follow-up of their patients. Nevertheless, current assessments of patients with chronic pain provide only fragmentary data on painful daily experiences. Real-life monitoring of subjective and objective markers of chronic pain using mobile health (mHealth) programs can address this issue.
Objective: We hypothesized that regular patient self-monitoring using an mHealth app would lead physicians to obtain deeper understanding and new insight into patients with chronic pain and that, for patients, regular self-monitoring using an mHealth app would play a positive therapeutic role and improve adherence to treatment. We aimed to evaluate the feasibility and acceptability of a new mHealth app called eDOL.
Methods: We conducted an observational study to assess the feasibility and acceptability of the eDOL tool. Patients completed several questionnaires using the tool over a period of 2 weeks and repeated assessments weekly over a period of 3 months. Physicians saw their patients at a follow-up visit that took place at least 3 months after the inclusion visit. A composite criterion of the acceptability and feasibility of the eDOL tool was calculated after the completion of study using satisfaction surveys from both patients and physicians.
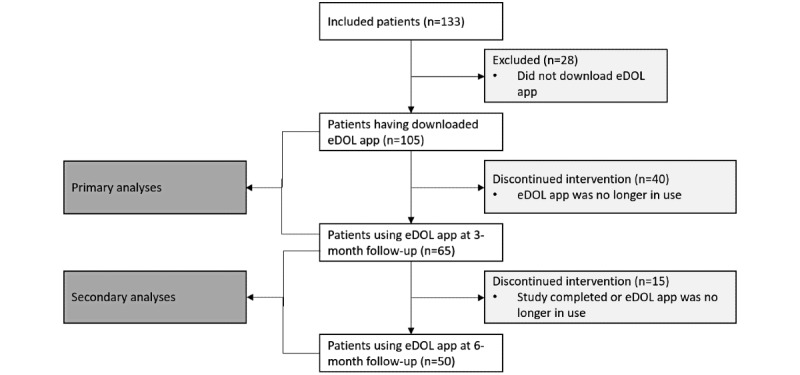
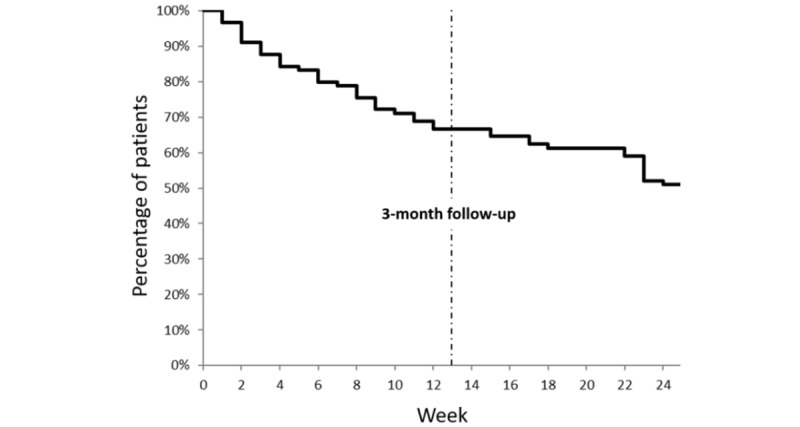
Results: Data from 105 patients (of 133 who were included) were analyzed. The rate of adherence was 61.9% (65/105) after 3 months. The median acceptability score was 7 (out of 10) for both patients and physicians. There was a high rate of completion of the baseline questionnaires and assessments (mean 89.3%), and a low rate of completion of the follow-up questionnaires and assessments (63.8% (67/105) and 61.9% (65/105) respectively). We were also able to characterize subgroups of patients and determine a profile of those who adhered to eDOL. We obtained 4 clusters that differ from each other in their biopsychosocial characteristics. Cluster 4 corresponds to patients with more disabling chronic pain (daily impact and comorbidities) and vice versa for cluster 1.
Conclusions: This work demonstrates that eDOL is highly feasible and acceptable for both patients with chronic pain and their physicians. It also shows that such a tool can integrate many parameters to ensure the detailed characterization of patients for future research works and pain management.
Trial registration: ClinicalTrial.gov NCT03931694; http://clinicaltrials.gov/ct2/show/NCT03931694.
Keywords: chronic pain; eHealth; feasibility study; mHealth; self-monitoring.
©Nicolas Kerckhove, Noémie Delage, Sébastien Cambier, Nathalie Cantagrel, Eric Serra, Fabienne Marcaillou, Caroline Maindet, Pascale Picard, Gaelle Martiné, Rodrigue Deleens, Anne-Priscille Trouvin, Lauriane Fourel, Gaelle Espagne-Dubreuilh, Ludovic Douay, Stéphane Foulon, Bénédicte Dufraisse, Christian Gov, Eric Viel, François Jedryka, Sophie Pouplin, Cécile Lestrade, Emmanuel Combe, Serge Perrot, Dominique Perocheau, Valentine De Brisson, Pascale Vergne-Salle, Patrick Mertens, Bruno Pereira, Abdoul Jalil Djiberou Mahamadou, Violaine Antoine, Alice Corteval, Alain Eschalier, Christian Dualé, Nadine Attal, Nicolas Authier. Originally published in JMIR Formative Research (https://formative.jmir.org), 02.03.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013 Jul;111(1):13–8. doi: 10.1093/bja/aet123. https://linkinghub.elsevier.com/retrieve/pii/S0007-0912(17)32961-6 S0007-0912(17)32961-6 - DOI - PubMed
-
- Docking RE, Fleming J, Brayne C, Zhao J, Macfarlane GJ, Jones GT, Cambridge City over-75s Cohort Study collaboration Epidemiology of back pain in older adults: prevalence and risk factors for back pain onset. Rheumatology (Oxford) 2011 Sep;50(9):1645–53. doi: 10.1093/rheumatology/ker175.ker175 - DOI - PubMed
-
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP) Pain. 2004 Jul;110(1-2):361–8. doi: 10.1016/j.pain.2004.04.017.S0304395904002076 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
