

Evaluation of Quality of Life After Nonoperative or Operative Management of Proximal Femoral Fractures in Frail Institutionalized Patients: The FRAIL-HIP Study
- PMID: 35234817
- PMCID: PMC8892372
- DOI: 10.1001/jamasurg.2022.0089
Evaluation of Quality of Life After Nonoperative or Operative Management of Proximal Femoral Fractures in Frail Institutionalized Patients: The FRAIL-HIP Study
Abstract
Importance: Decision-making on management of proximal femoral fractures in frail patients with limited life expectancy is challenging, but surgical overtreatment needs to be prevented. Current literature provides limited insight into the true outcomes of nonoperative management and operative management in this patient population.
Objective: To investigate the outcomes of nonoperative management vs operative management of proximal femoral fractures in institutionalized frail older patients with limited life expectancy.
Design, setting, and participants: This multicenter cohort study was conducted between September 1, 2018, and April 25, 2020, with a 6-month follow-up period at 25 hospitals across the Netherlands. Eligible patients were aged 70 years or older, frail, and institutionalized and sustained a femoral neck or pertrochanteric fracture. The term frail implied at least 1 of the following characteristics was present: malnutrition (body mass index [calculated as weight in kilograms divided by height in meters squared] <18.5) or cachexia, severe comorbidities (American Society of Anesthesiologists physical status class of IV or V), or severe mobility issues (Functional Ambulation Category ≤2).
Exposures: Shared decision-making (SDM) followed by nonoperative or operative fracture management.
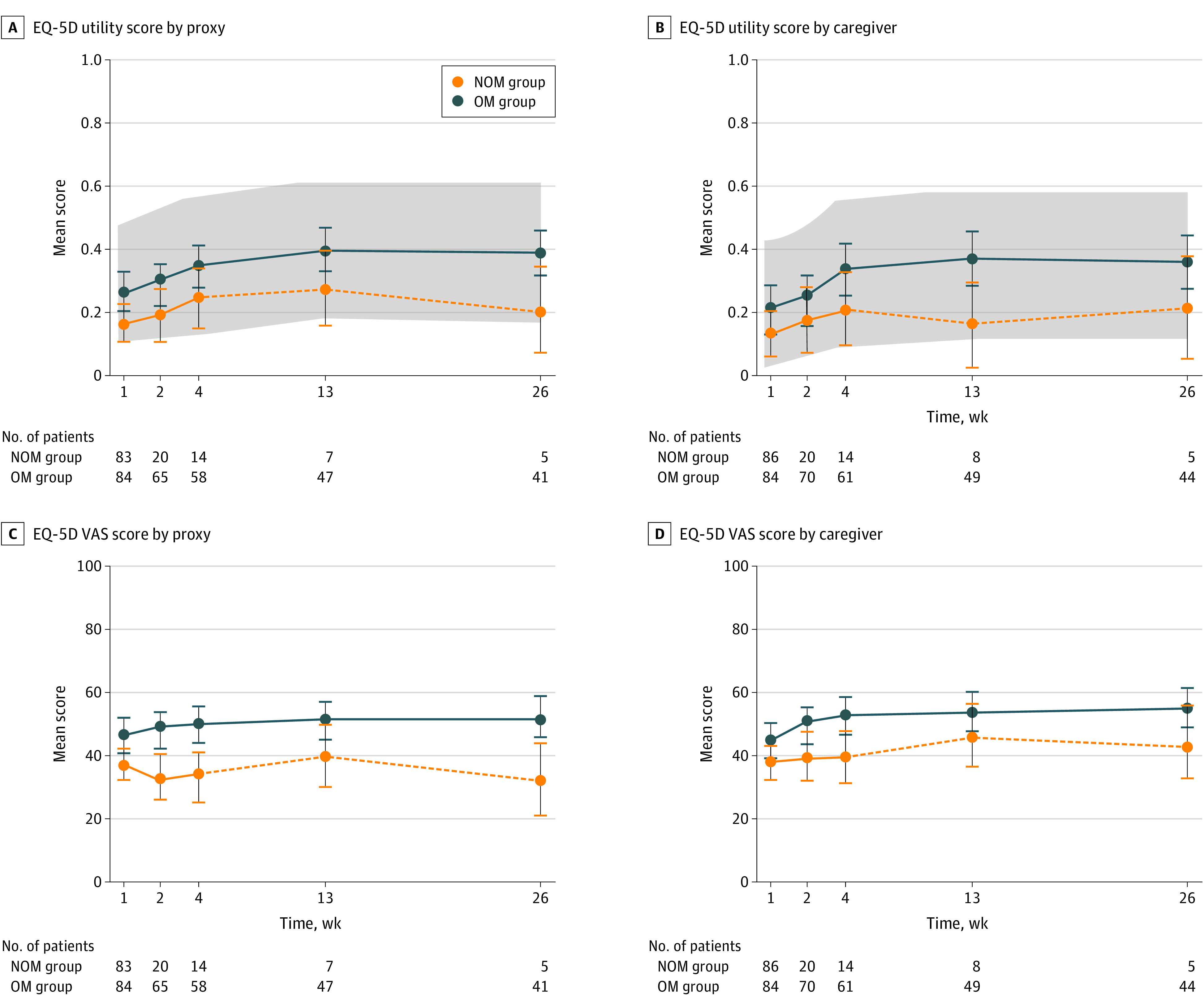
Main outcomes and measures: The primary outcome was the EuroQol 5 Dimension 5 Level (EQ-5D) utility score by proxies and caregivers. Secondary outcome measures were QUALIDEM (a dementia-specific quality-of-life instrument for persons with dementia in residential settings) scores, pain level (assessed by the Pain Assessment Checklist for Seniors With Limited Ability to Communicate), adverse events (Clavien-Dindo classification), mortality, treatment satisfaction (numeric rating scale), and quality of dying (Quality of Dying and Death Questionnaire).
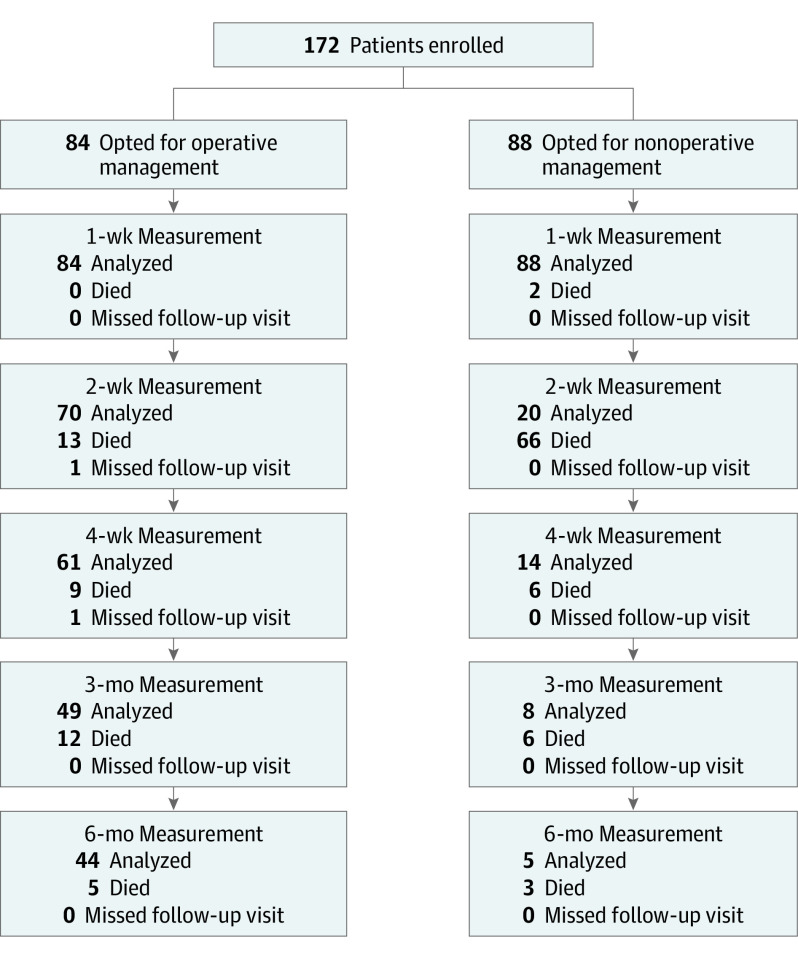
Results: Of the 172 enrolled patients with proximal femoral fractures (median [25th and 75th percentile] age, 88 [85-92] years; 135 women [78%]), 88 opted for nonoperative management and 84 opted for operative management. The EQ-5D utility scores by proxies and caregivers in the nonoperative management group remained within the set 0.15 noninferiority limit of the operative management group (week 1: 0.17 [95% CI, 0.13-0.29] vs 0.26 [95% CI, 0.11-0.23]; week 2: 0.19 [95% CI, 0.10-0.27] vs 0.28 [95% CI, 0.22-0.35]; and week 4: 0.24 [95% CI, 0.15-0.33] vs 0.34 [95% CI, 0.28-0.41]). Adverse events were less frequent in the nonoperative management group vs the operative management group (67 vs 167). The 30-day mortality rate was 83% (n = 73) in the nonoperative management group and 25% (n = 21) in the operative management group, with 26 proxies and caregivers (51%) in the nonoperative management group rating the quality of dying as good-almost perfect. Treatment satisfaction was high in both groups, with a median numeric rating scale score of 8.
Conclusions and relevance: Results of this study indicated that nonoperative management of proximal femoral fractures (selected through an SDM process) was a viable option for frail institutionalized patients with limited life expectancy, suggesting that surgery should not be a foregone conclusion for this patient population.
Conflict of interest statement
Figures
Comment in
-
A Holistic Approach for Treating Fragility Fractures in Older Adults.JAMA Surg. 2022 May 1;157(5):434-435. doi: 10.1001/jamasurg.2022.0114. JAMA Surg. 2022. PMID: 35234823 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
