

Reinforcement Learning in Patients With Mood and Anxiety Disorders vs Control Individuals: A Systematic Review and Meta-analysis
- PMID: 35234834
- PMCID: PMC8892374
- DOI: 10.1001/jamapsychiatry.2022.0051
Reinforcement Learning in Patients With Mood and Anxiety Disorders vs Control Individuals: A Systematic Review and Meta-analysis
Abstract
Importance: Computational psychiatry studies have investigated how reinforcement learning may be different in individuals with mood and anxiety disorders compared with control individuals, but results are inconsistent.
Objective: To assess whether there are consistent differences in reinforcement-learning parameters between patients with depression or anxiety and control individuals.
Data sources: Web of Knowledge, PubMed, Embase, and Google Scholar searches were performed between November 15, 2019, and December 6, 2019, and repeated on December 3, 2020, and February 23, 2021, with keywords (reinforcement learning) AND (computational OR model) AND (depression OR anxiety OR mood).
Study selection: Studies were included if they fit reinforcement-learning models to human choice data from a cognitive task with rewards or punishments, had a case-control design including participants with mood and/or anxiety disorders and healthy control individuals, and included sufficient information about all parameters in the models.
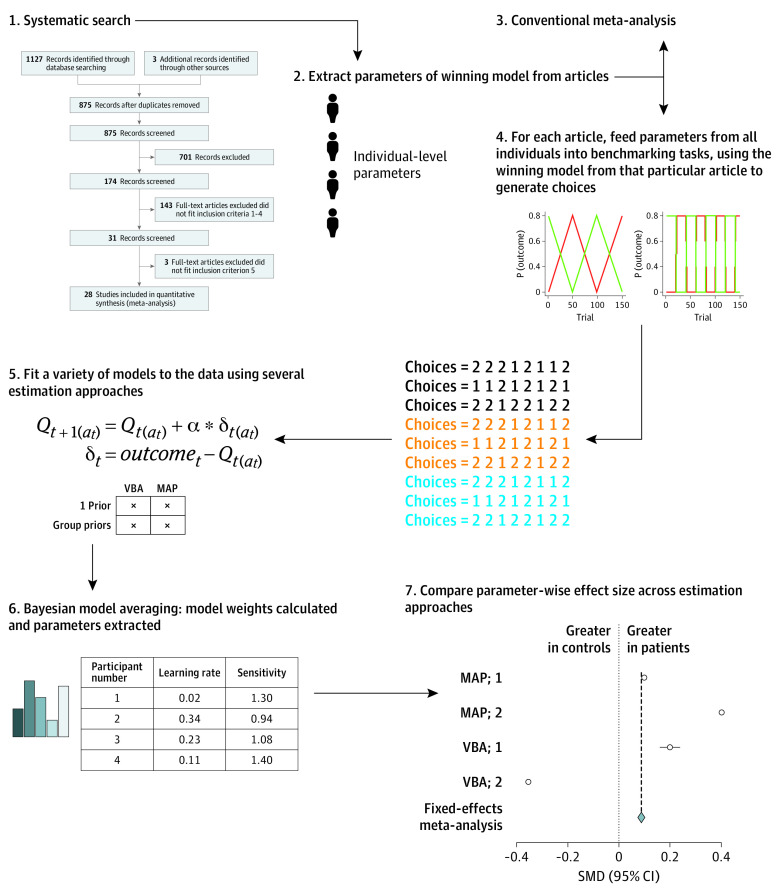
Data extraction and synthesis: Articles were assessed for inclusion according to MOOSE guidelines. Participant-level parameters were extracted from included articles, and a conventional meta-analysis was performed using a random-effects model. Subsequently, these parameters were used to simulate choice performance for each participant on benchmarking tasks in a simulation meta-analysis. Models were fitted, parameters were extracted using bayesian model averaging, and differences between patients and control individuals were examined. Overall effect sizes across analytic strategies were inspected.
Main outcomes and measures: The primary outcomes were estimated reinforcement-learning parameters (learning rate, inverse temperature, reward learning rate, and punishment learning rate).
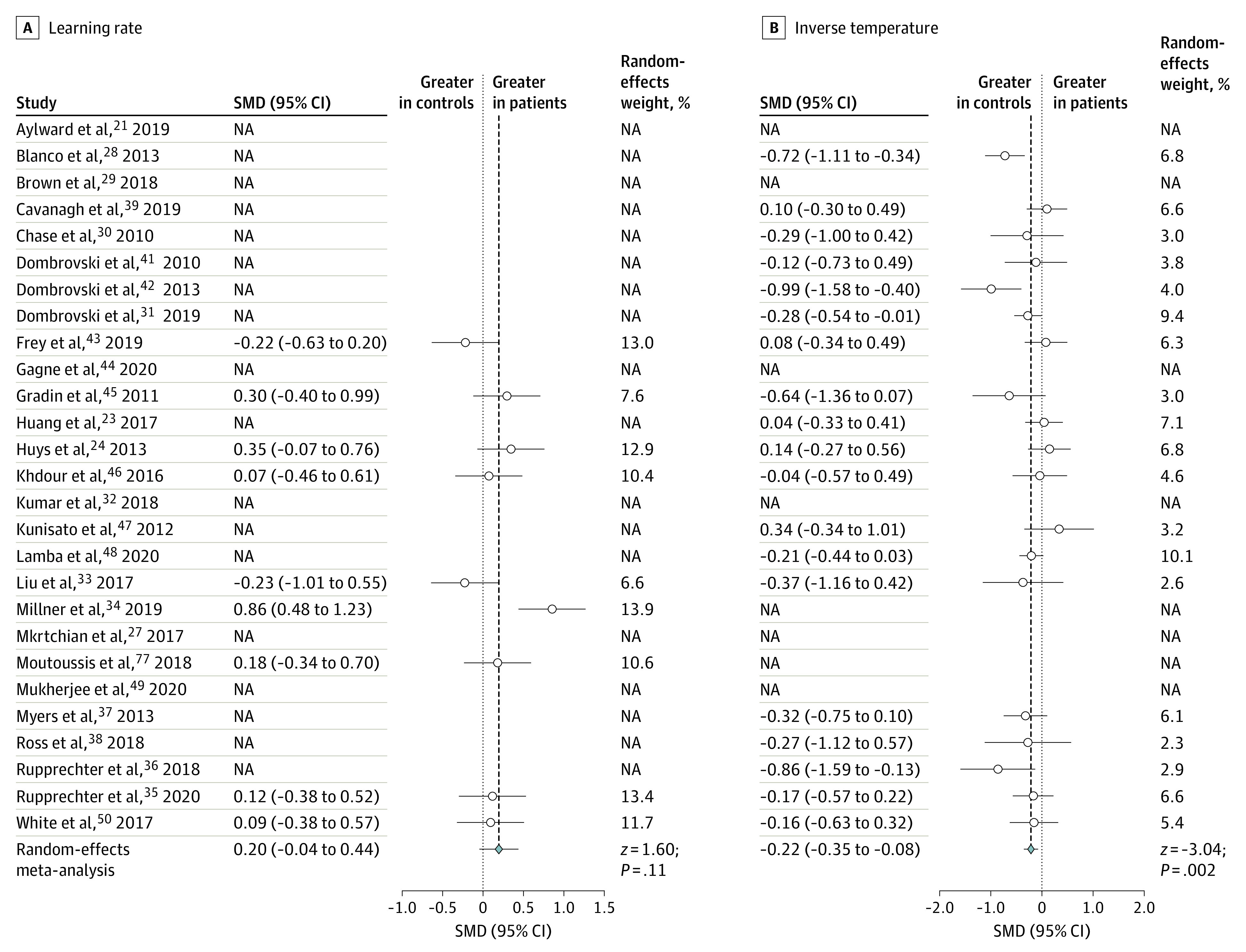
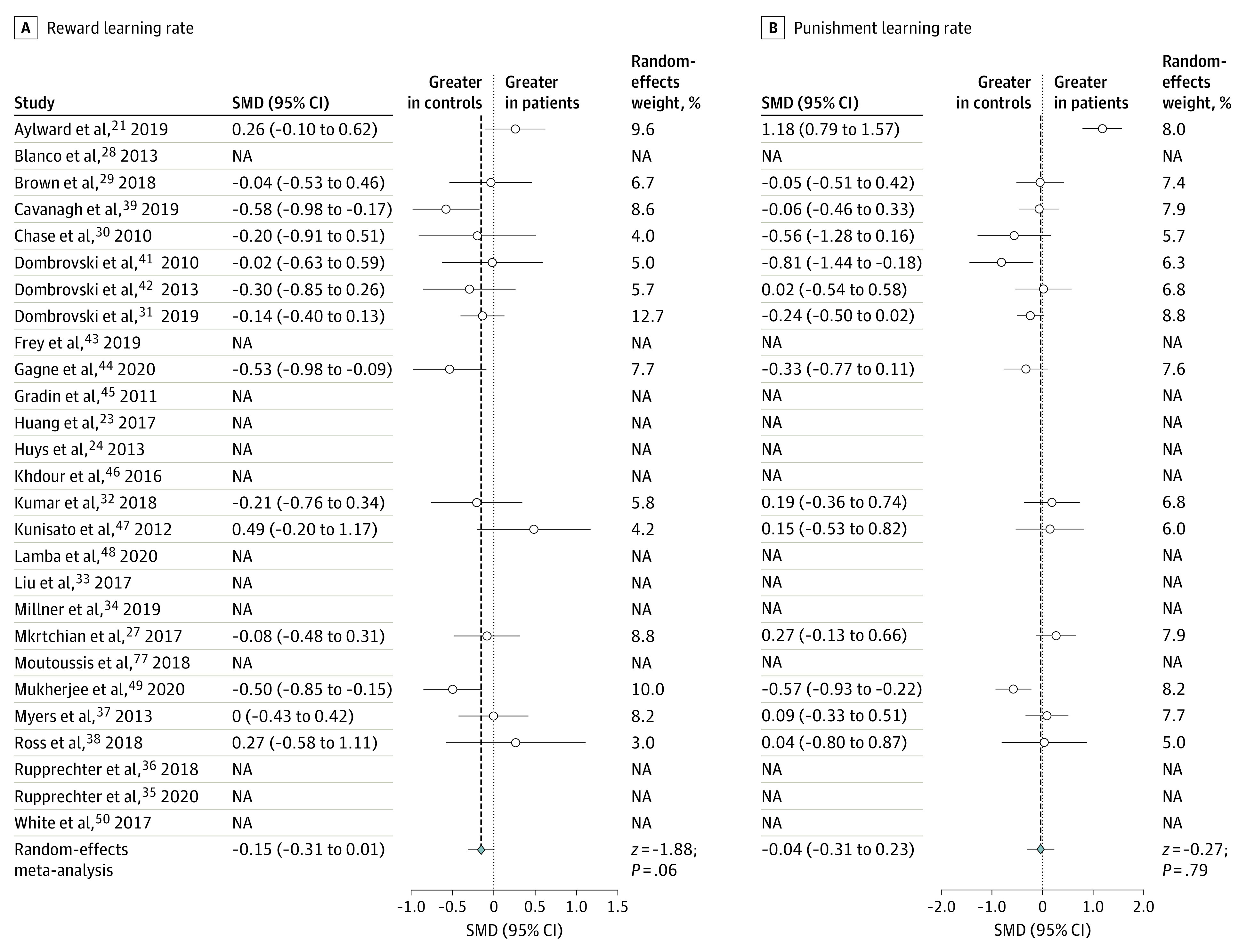
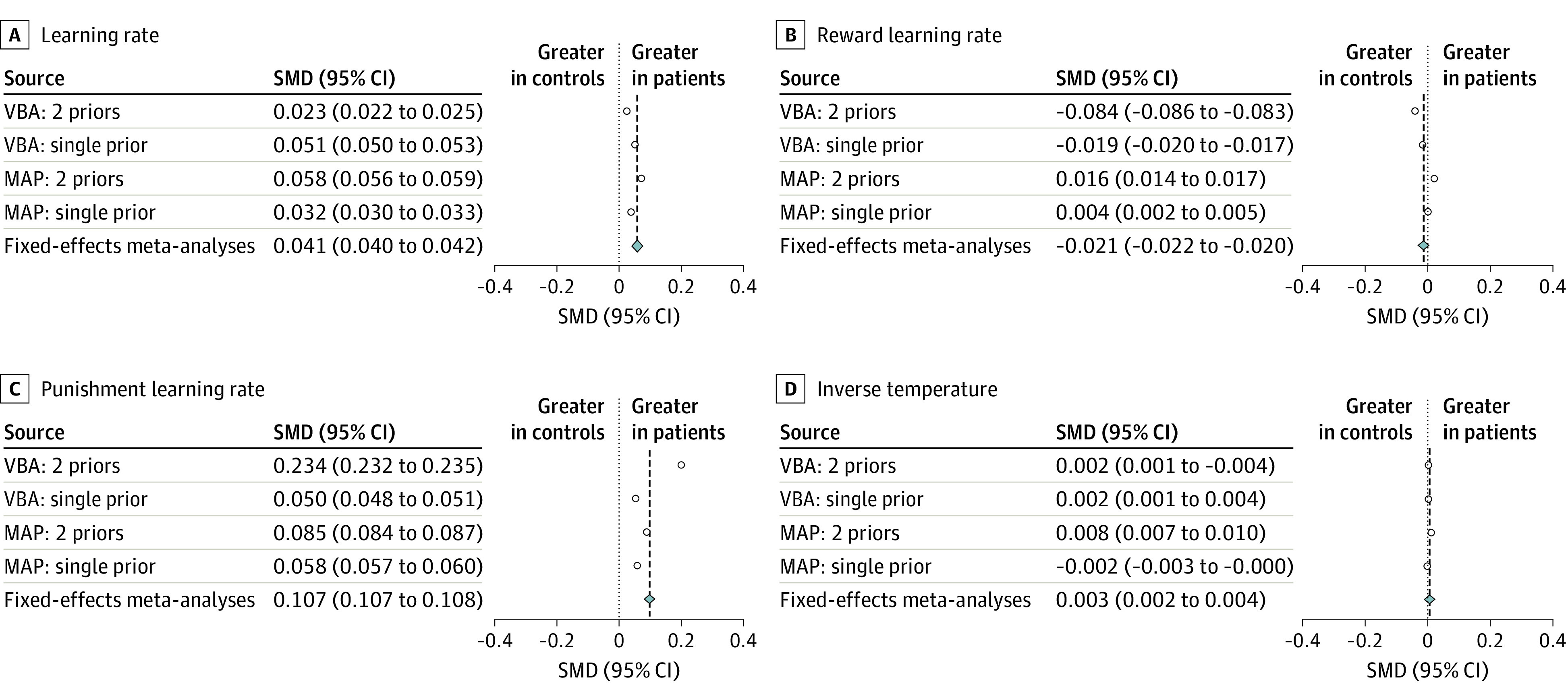
Results: A total of 27 articles were included (3085 participants, 1242 of whom had depression and/or anxiety). In the conventional meta-analysis, patients showed lower inverse temperature than control individuals (standardized mean difference [SMD], -0.215; 95% CI, -0.354 to -0.077), although no parameters were common across all studies, limiting the ability to infer differences. In the simulation meta-analysis, patients showed greater punishment learning rates (SMD, 0.107; 95% CI, 0.107 to 0.108) and slightly lower reward learning rates (SMD, -0.021; 95% CI, -0.022 to -0.020) relative to control individuals. The simulation meta-analysis showed no meaningful difference in inverse temperature between patients and control individuals (SMD, 0.003; 95% CI, 0.002 to 0.004).
Conclusions and relevance: The simulation meta-analytic approach introduced in this article for inferring meta-group differences from heterogeneous computational psychiatry studies indicated elevated punishment learning rates in patients compared with control individuals. This difference may promote and uphold negative affective bias symptoms and hence constitute a potential mechanistic treatment target for mood and anxiety disorders.
Conflict of interest statement
Figures
References
-
- Kyu HH, Abate D, Abate KH, et al. ; GBD 2017 DALYs and HALE Collaborators . Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859-1922. doi:10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- NHS Digital . Psychological therapies, annual report on the use of IAPT services 2018-19. Published July 11, 2019. Accessed May 14, 2020. https://digital.nhs.uk/data-and-information/publications/statistical/psy...
