

Prenatal dexamethasone treatment for classic 21-hydroxylase deficiency in Europe
- PMID: 35235536
- PMCID: PMC9010809
- DOI: 10.1530/EJE-21-0554
Prenatal dexamethasone treatment for classic 21-hydroxylase deficiency in Europe
Abstract
Objective: To assess the current medical practice in Europe regarding prenatal dexamethasone (Pdex) treatment of congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency.
Design and methods: A questionnaire was designed and distributed, including 17 questions collecting quantitative and qualitative data. Thirty-six medical centres from 14 European countries responded and 30 out of 36 centres were reference centres of the European Reference Network on Rare Endocrine Conditions, EndoERN.
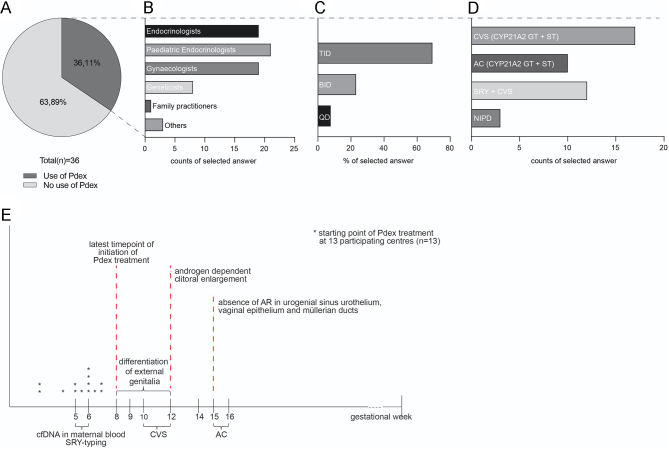
Results: Pdex treatment is currently provided by 36% of the surveyed centres. The treatment is initiated by different specialties, that is paediatricians, endocrinologists, gynaecologists or geneticists. Regarding the starting point of Pdex, 23% stated to initiate therapy at 4-5 weeks postconception (wpc), 31% at 6 wpc and 46 % as early as pregnancy is confirmed and before 7 wpc at the latest. A dose of 20 µg/kg/day is used. Dose distribution among the centres varies from once to thrice daily. Prenatal diagnostics for treated cases are conducted in 72% of the responding centres. Cases treated per country and year vary between 0.5 and 8.25. Registries for long-term follow-up are only available at 46% of the centres that are using Pdex treatment. National registries are only available in Sweden and France.
Conclusions: This study reveals a high international variability and discrepancy in the use of Pdex treatment across Europe. It highlights the importance of a European cooperation initiative for a joint international prospective trial to establish evidence-based guidelines on prenatal diagnostics, treatment and follow-up of pregnancies at risk for CAH.
Figures
References
-
- Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HF, Miller WL, Montori VM, Oberfield SEet al. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology and Metabolism 2010954133–4160. ( 10.1210/jc.2009-2631) - DOI - PMC - PubMed
