

Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living With Human Immunodeficiency Virus 1 (HIV-1): Week 48 Results From the Phase 3, Noninferiority SALSA Randomized Trial
- PMID: 35235656
- PMCID: PMC10021070
- DOI: 10.1093/cid/ciac130
Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living With Human Immunodeficiency Virus 1 (HIV-1): Week 48 Results From the Phase 3, Noninferiority SALSA Randomized Trial
Abstract
Background: In TANGO, switching to dolutegravir/lamivudine (DTG/3TC) demonstrated long-term noninferior efficacy vs continuing tenofovir alafenamide-based regimens in treatment-experienced adults with HIV-1. The phase 3 SALSA study evaluated efficacy and safety of switching to DTG/3TC compared with continuing various 3-/4-drug current antiretroviral regimens (CARs).
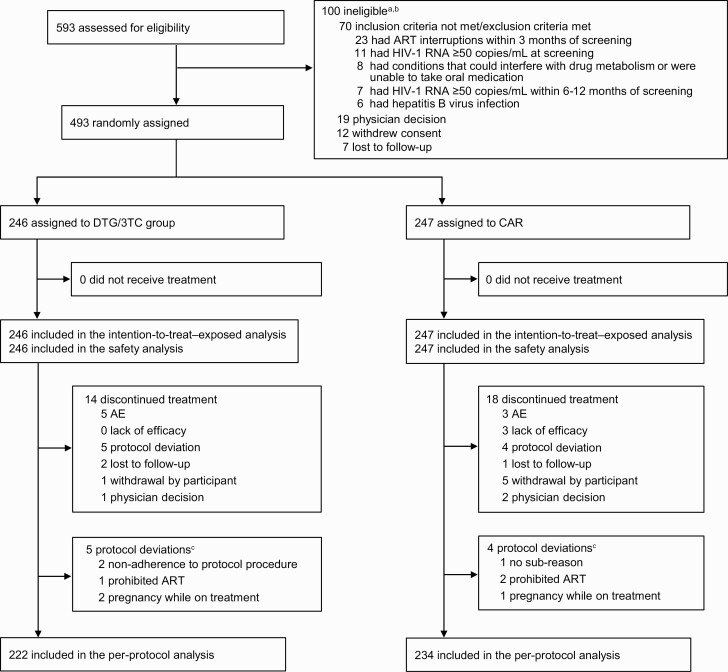
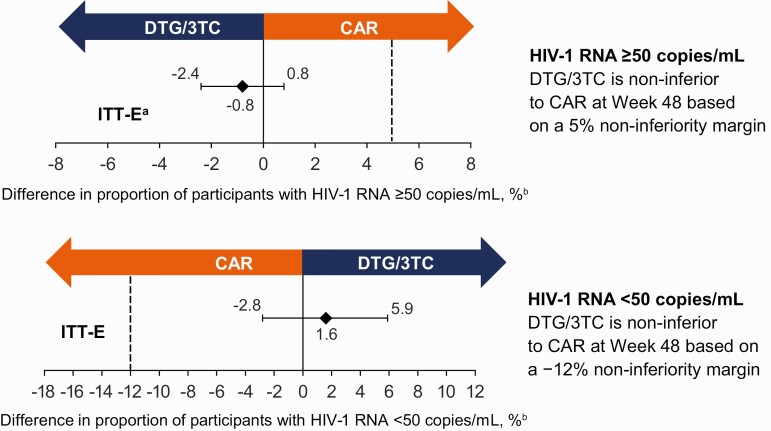
Methods: Adults with HIV-1 RNA <50 copies/mL and no previous virologic failure were randomized (1:1, stratified by baseline third agent class) to switch to once-daily fixed-dose combination DTG/3TC or continue CAR (primary endpoint: proportion of participants with HIV-1 RNA ≥50 copies/mL at week 48; Snapshot, intention-to-treat-exposed population, 5% noninferiority margin).
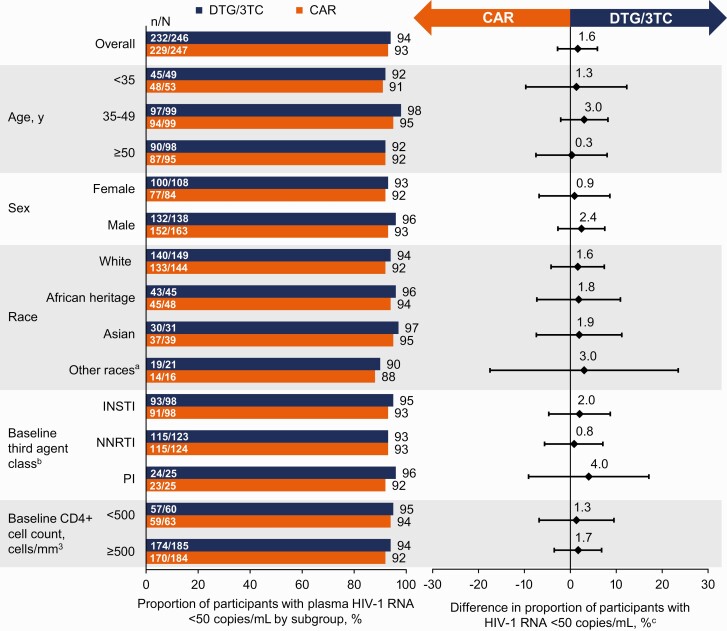
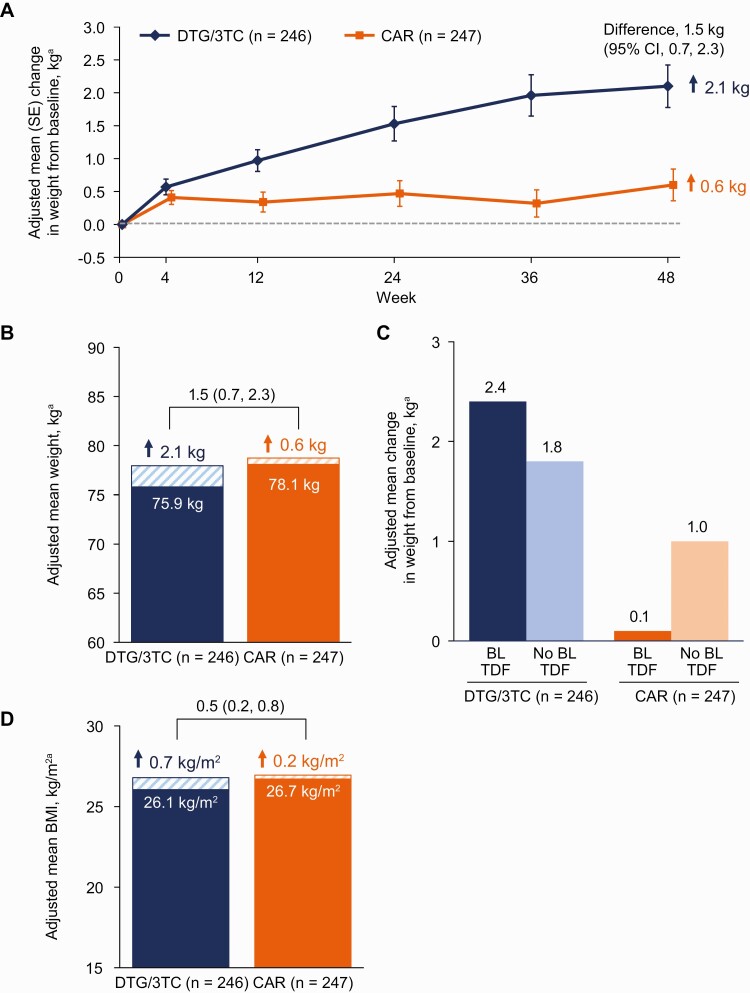
Results: Overall, 493 adults (39% women; 39% aged ≥50 years; 19% African American/African heritage; 14% Asian) were randomized to switch to DTG/3TC (n = 246) or continue CAR (n = 247). At week 48, 1 (0.4%) participant in the DTG/3TC group and 3 (1.2%) in the CAR group had HIV-1 RNA ≥50 copies/mL (Snapshot), demonstrating noninferiority (adjusted difference, -0.8%; 95% CI, -2.4%, .8%). Zero participants met confirmed virologic withdrawal criteria; therefore, no resistance testing was performed. Drug-related adverse events were more frequent with DTG/3TC (20%) than CAR (6%) through week 48 but comparable post-week 24 (5% vs 2%, respectively). Proximal tubular renal function and bone turnover biomarkers improved with DTG/3TC. Both groups had generally minimal changes in lipids and inflammatory biomarkers.
Conclusions: Switching to DTG/3TC was noninferior to continuing CAR for maintaining virologic suppression at week 48 with no observed resistance, supporting the efficacy, good safety, and high barrier to resistance of DTG/3TC.
Clinical trials registration: www.clinicaltrials.gov, NCT04021290.
Keywords: 2-drug regimen; dolutegravir/lamivudine; integrase strand transfer inhibitor; treatment-experienced; virologic suppression.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. J. M. L. has received honoraria or consultation fees from and participated in company-sponsored speakers bureaus for ViiV Healthcare, Gilead, and Janssen-Cilag. C. B. has received grants for an investigator-initiated study from GSK and honoraria for presentations from GSK, Gilead, and Merck Sharpe and Dohme; and has participated in advisory boards for GSK and Gilead. L. H. has received fees for participation in advisory boards or presentations from ViiV Healthcare, Merck Sharpe and Dohme, and Gilead and has received travel support for congress attendance from ViiV Healthcare, Merck Sharpe and Dohme, and Gilead. O. O. has received honoraria from ViiV Healthcare and Gilead. C. G. has received consulting fees and honoraria from ViiV Healthcare, Gilead, Merck Sharp and Dohme, and Janssen and has received support for meeting attendance from Gilead and Janssen. F. M. has received grants from ViiV Healthcare, Gilead, and Janssen, which were paid to his institution; has received honoraria from ViiV Healthcare, Gilead, Janssen, and Merck Sharp and Dohme; and has participated in data safety monitoring/advisory boards for ViiV Healthcare, Gilead, Janssen, and Merck Sharp and Dohme. S. T. has received grants for investigator-initiated studies from Gilead; has participated in and received honoraria for advisory boards or company-sponsored speakers bureaus from ViiV Healthcare, Gilead, and Merck Sharp and Dohme; has received support for registration at scientific conferences from ViiV Healthcare; and is the unpaid Medical Director of Saving Lives. E. B., C. M., B. W., M. U., G. B., and J. v. W. are employees of ViiV Healthcare and may own stock in GSK. J. O. and L. C. are employees of and may own stock in GSK. C.-Y. C. and O. D. report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. 2021. Available at: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/ad.... Accessed 24 September 2021.
-
- European AIDS Clinical Society. EACS guidelines version 11.0. October 2021. Available at: https://www.eacsociety.org/media/final2021eacsguidelinesv11.0_oct2021.pdf. Accessed 7 November 2021.
-
- van Wyk J, Ajana F, Bisshop F, et al. . Switching to DTG/3TC fixed-dose combination (FDC) is non-inferior to continuing a TAF-based regimen (TBR) in maintaining virologic suppression through 96 weeks (TANGO study) [abstract O441]. In: Program and abstracts of HIV Drug Therapy Glasgow 2020 (virtual). Geneva, Switzerland: International AIDS Society, 2020:14.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
