

Does negative pressure wound therapy reduce the odds of infection and improve health-related quality of life in patients with open fractures?
- PMID: 35236110
- PMCID: PMC8965780
- DOI: 10.1302/2633-1462.33.BJO-2021-0199.R1
Does negative pressure wound therapy reduce the odds of infection and improve health-related quality of life in patients with open fractures?
Abstract
Aims: To evaluate the impact of negative pressure wound therapy (NPWT) on the odds of having deep infections and health-related quality of life (HRQoL) following open fractures.
Methods: Patients from the Fluid Lavage in Open Fracture Wounds (FLOW) trial with Gustilo-Anderson grade II or III open fractures within the lower limb were included in this secondary analysis. Using mixed effects logistic regression, we assessed the impact of NPWT on deep wound infection requiring surgical intervention within 12 months post-injury. Using multilevel model analyses, we evaluated the impact of NPWT on the Physical Component Summary (PCS) of the 12-Item Short-Form Health Survey (SF-12) at 12 months post-injury.
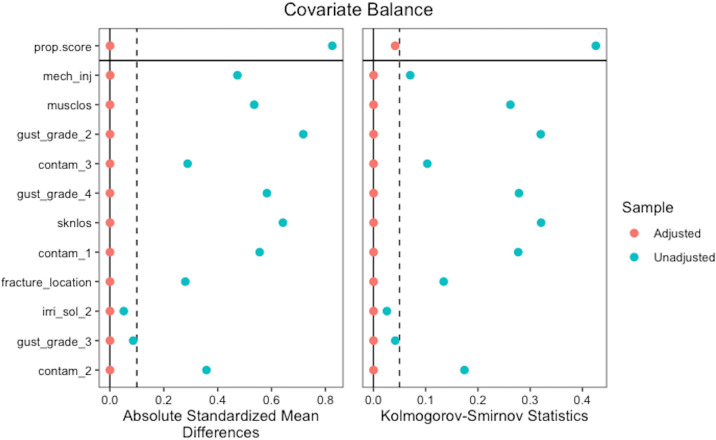
Results: After applying inverse probability treatment weighting to adjust for the influence of injury characteristics on type of dressing used, 1,322 participants were assessed. The odds of developing a deep infection requiring operative management within 12 months of initial surgery was 4.52-times higher in patients who received NPWT compared to those who received a standard wound dressing (95% confidence interval (CI) 1.84 to 11.12; p = 0.001). Overall, 1,040 participants were included in our HRQoL analysis, and those treated with NPWT had statistically significantly lower mean SF-12 PCS post-fracture (p < 0.001). These differences did not reach the minimally important difference for the SF-12 PCS.
Conclusion: Our analysis found that patients treated with NPWT had higher odds of developing a deep infection requiring operative management within 12 months post-fracture. Due to possible residual confounding with the worst cases being treated with NPWT, we are unable to determine if NPWT has a negative effect or is simply a marker of worse injuries or poor access to early soft-tissue coverage. Regardless, our results suggest that the use of this treatment requires further evaluation. Cite this article: Bone Jt Open 2022;3(3):189-195.
Keywords: Fractures; Infection; Negative Pressure Wound Therapy; SF-12 scores; Short Form Health Survey; deep infections; infection; logistic regression analysis; negative pressure wound therapy; open fractures; physical component summary (PCS); soft-tissue; wounds.
Conflict of interest statement
Figures
References
-
- Hull PD, Johnson SC, Stephen DJG, Kreder HJ, Jenkinson RJ. Delayed debridement of severe open fractures is associated with a higher rate of deep infection. Bone Joint J. 2014;96-B(3):379–384. - PubMed
-
- Westgeest J, Weber D, Dulai SK, Bergman JW, Buckley R, Beaupre LA. Factors associated with development of nonunion or delayed healing after an open long bone fracture: a prospective cohort study of 736 subjects. J Orthop Trauma. 2016;30(3):149–155. - PubMed
-
- MacKenzie EJ, Jones AS, Bosse MJ, et al. . Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007;89-A(8):1685–1692. - PubMed
-
- Sprague S, Bhandari M, Heetveld MJ, et al. . Factors associated with health-related quality of life, hip function, and health utility after operative management of femoral neck fractures. Bone Joint J. 2018;100-B(3):361–369. - PubMed
