

Treatment regimens for neuromyelitis optica spectrum disorder attacks: a retrospective cohort study
- PMID: 35236386
- PMCID: PMC8892703
- DOI: 10.1186/s12974-022-02420-2
Treatment regimens for neuromyelitis optica spectrum disorder attacks: a retrospective cohort study
Abstract
Background: Neuromyelitis optica spectrum disorder (NMOSD) attacks require an urgent probabilistic anti-inflammatory therapeutic strategy. As inadequately treated attacks result in disability, there is a need to identify the optimal attack-treatment regimen. Our study aimed to identify predictors of outcome after a first attack in patients with an NMOSD presentation and propose the best treatment strategy.
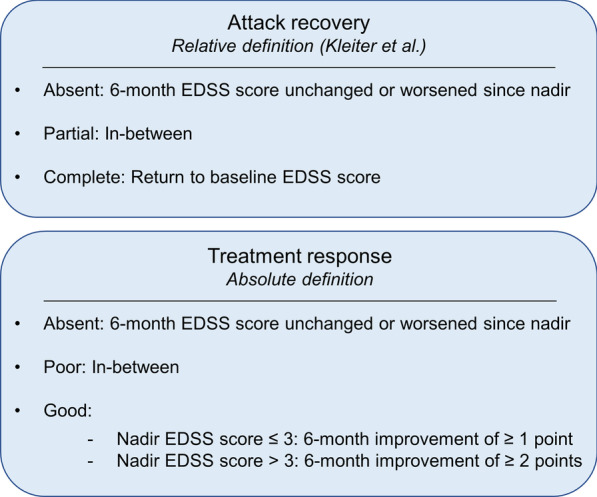
Methods: We performed a retrospective cohort study on the French national NMOSD registry (NOMADMUS), a nested cohort of the French multiple sclerosis observatory (OFSEP) recruiting patients with NMOSD presentations in France. We studied the first attack for any independent locations of clinical core characteristic of NMOSD, in treatment-naïve patients. The primary outcome was the evolution of the Expanded Disability Status Scale (EDSS) score at 6 months, stratified in two ways to account for recovery (return to baseline EDSS score) and treatment response (classified as "good" if the EDSS score decreased by ≥ 1 point after a nadir EDSS score ≤ 3, or by ≥ 2 points after a nadir EDSS score > 3). We used ordinal logistic regression to infer statistical associations with the outcome.
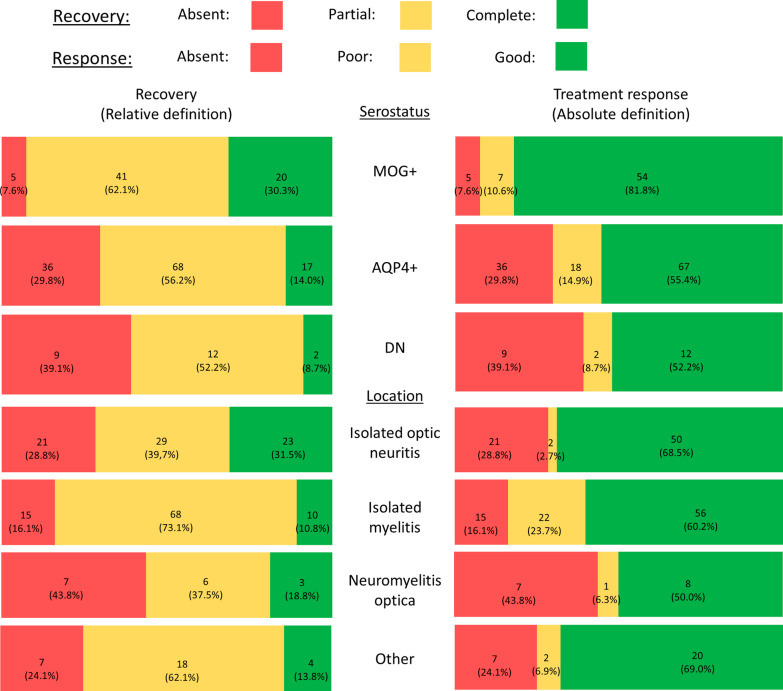
Results: We included 211 attacks among 183 patients (104 with anti-AQP4 antibodies, 60 with anti-MOG antibodies, and 19 double seronegative). Attack treatment regimens comprised corticosteroids (n = 196), plasma exchanges (PE; n = 72) and intravenous immunoglobulins (n = 6). Complete recovery was reached in 40 attacks (19%) at 6 months. The treatment response was "good" in 134 attacks (63.5%). There was no improvement in EDSS score in 50 attacks (23.7%). MOG-antibody seropositivity and short delays to PE were significantly and independently associated with better recovery and treatment response.
Conclusions: We identified two prognostic factors: serostatus (with better outcomes among MOG-Ab-positive patients) and the delay to PE. We, therefore, argue for a more aggressive anti-inflammatory management of the first attacks suggesting an NMOSD presentation, with the early combination of PE with corticosteroids.
Keywords: Corticosteroids; MOGAD; Neuromyelitis optica; Plasma exchanges; Relapses; Therapeutics.
© 2022. The Author(s).
Conflict of interest statement
HZ has received honoraria from Biogen IDEC, Novartis, Merck, Roche, Alexion, support for travelling from Biogen, Novartis, Merck and Roche. She serves on the advisory board of Novartis. Her institution perceived a grant from Roche. SV reports honoraria from Biogen, Celgene, Merck, Novartis, Roche, Sanofi paid to her institution. EM has received grants or contracts from Roche and Biogen to her institution. She has received consulting fees and support for travelling from Roche, Biogen, Novartis, Merck, Sanofi-genzyme, Teva, Alexion. MC serves on the scientific advisory board for Biogen, Teva, Novartis, Sanofi, Roche, Ad Scientiam and Alexion. RM serves on the scientific advisory board for Viela Bio, Roche, UCB, and Alexion, and has received honoraria from Biogen, Merck, and Novartis. NC serves on scientific advisory boards for, and has received honoraria from, Biogen Idec, Merck Serono, Sanofi-Genzyme, Bayer Schering Pharma, and Alexion Pharmaceutical. SD, MG, BB, JC, YS, AK, CLF, CP, LM, DL and BA reports no disclosures.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
