

Detection of COVID-19 using multimodal data from a wearable device: results from the first TemPredict Study
- PMID: 35236896
- PMCID: PMC8891385
- DOI: 10.1038/s41598-022-07314-0
Detection of COVID-19 using multimodal data from a wearable device: results from the first TemPredict Study
Erratum in
-
Author Correction: Detection of COVID-19 using multimodal data from a wearable device: results from the first TemPredict Study.Sci Rep. 2022 Mar 16;12(1):4568. doi: 10.1038/s41598-022-08723-x. Sci Rep. 2022. PMID: 35296773 Free PMC article. No abstract available.
Abstract
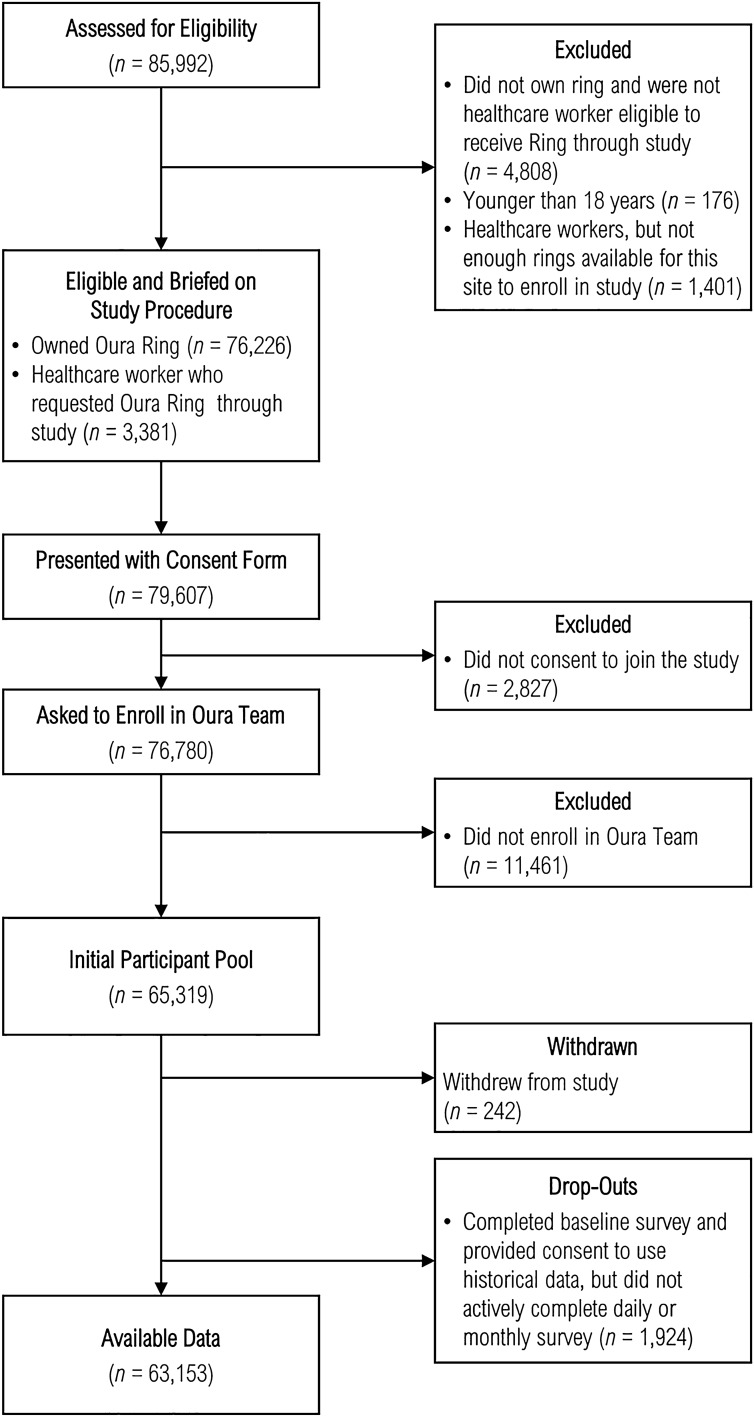
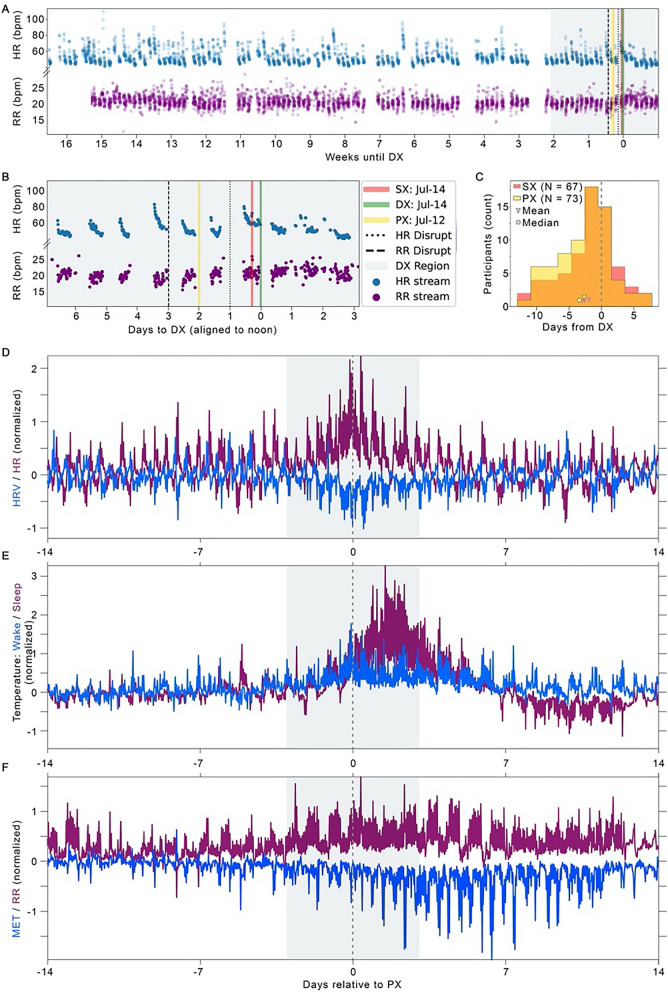
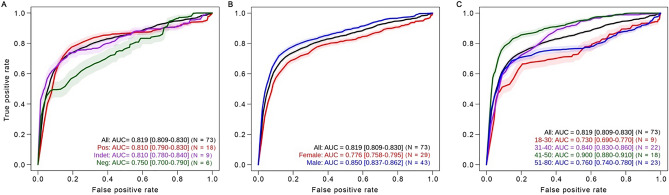
Early detection of diseases such as COVID-19 could be a critical tool in reducing disease transmission by helping individuals recognize when they should self-isolate, seek testing, and obtain early medical intervention. Consumer wearable devices that continuously measure physiological metrics hold promise as tools for early illness detection. We gathered daily questionnaire data and physiological data using a consumer wearable (Oura Ring) from 63,153 participants, of whom 704 self-reported possible COVID-19 disease. We selected 73 of these 704 participants with reliable confirmation of COVID-19 by PCR testing and high-quality physiological data for algorithm training to identify onset of COVID-19 using machine learning classification. The algorithm identified COVID-19 an average of 2.75 days before participants sought diagnostic testing with a sensitivity of 82% and specificity of 63%. The receiving operating characteristic (ROC) area under the curve (AUC) was 0.819 (95% CI [0.809, 0.830]). Including continuous temperature yielded an AUC 4.9% higher than without this feature. For further validation, we obtained SARS CoV-2 antibody in a subset of participants and identified 10 additional participants who self-reported COVID-19 disease with antibody confirmation. The algorithm had an overall ROC AUC of 0.819 (95% CI [0.809, 0.830]), with a sensitivity of 90% and specificity of 80% in these additional participants. Finally, we observed substantial variation in accuracy based on age and biological sex. Findings highlight the importance of including temperature assessment, using continuous physiological features for alignment, and including diverse populations in algorithm development to optimize accuracy in COVID-19 detection from wearables.
© 2022. The Author(s).
Conflict of interest statement
Co-Authors Affiliated with the MIT Lincoln Laboratory: Patent US 10332638 was issued to MIT in June 2019 and covers aspects of the physiological data pre-processing and classifier training and testing. Patent inventors: A. Swiston, T. Patel, L. Milechin, J. Fleischman, W. Pratt, and A. Honko. None of the patent inventors are authors on this manuscript. Elissa S. Epel, PhD Dr. Epel has received loaned equipment from Oura Health to conduct research using Oura Rings. Ashley Mason, PhD, and Benjamin Smarr, PhD Patent applications US App. No. 17/357,922, US App. No. 17/357,930, and PCT App. No. PCT/US21/39260 have been filed as of July 2021 by Ōura Health Oy on behalf of UCSD. All applications cover use of wearable device data to detect illness onset. Authors A. Mason and B. Smarr are listed as co-inventors on these applications. Benjamin Smarr, PhD Dr. Smarr has received remuneration for consulting work from, and has a financial interest in Oura Ring Inc. Other authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
