

The Reliability of CT Scan Measurements of Pelvic Incidence in the Evaluation of Adult Spondylolisthesis
- PMID: 35237488
- PMCID: PMC8882350
- DOI: 10.7759/cureus.21696
The Reliability of CT Scan Measurements of Pelvic Incidence in the Evaluation of Adult Spondylolisthesis
Abstract
Background: Pelvic incidence (PI) has been described as a parameter that may be a risk factor for lumbar spondylolisthesis (SPL). Studies have reported PI measurement is more precise in CT scans. Very limited studies have measured PI using CT scans to evaluate SPL. We analyzed the reliability of CT scans to measure PI to evaluate SPL and compared it to patients without SPL.
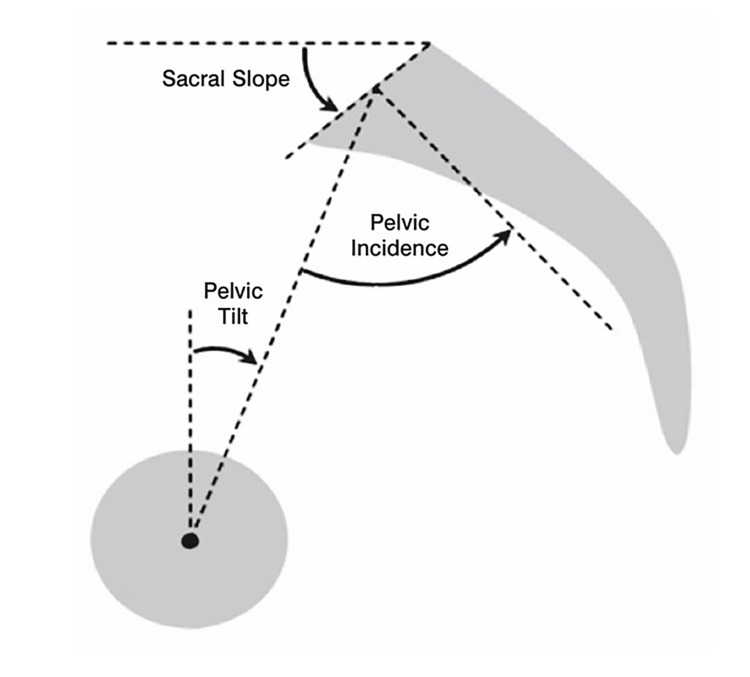
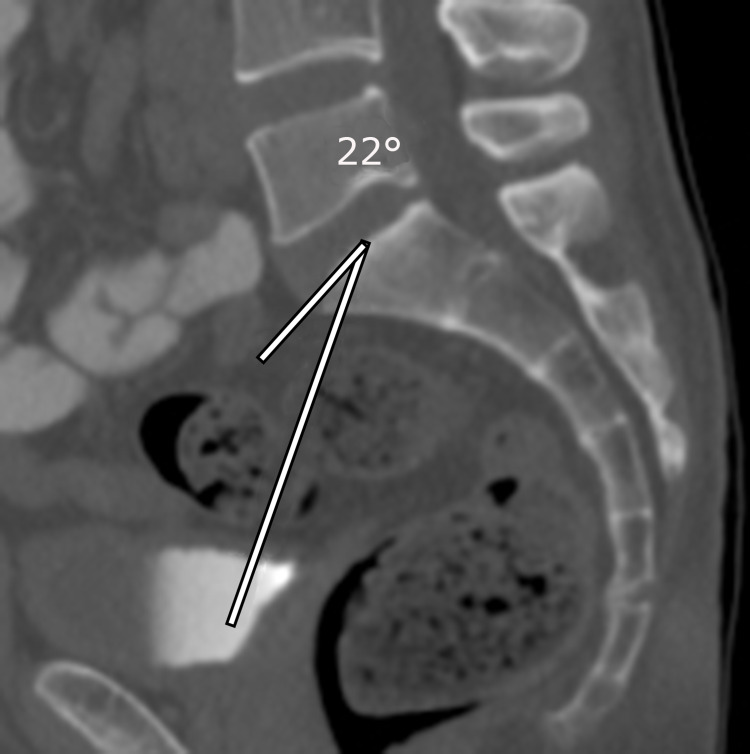
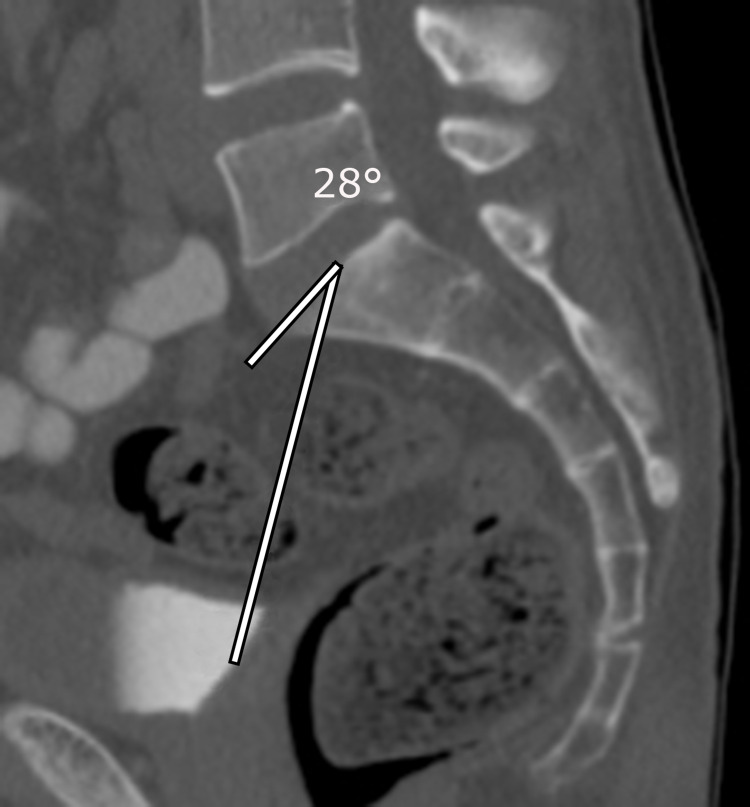
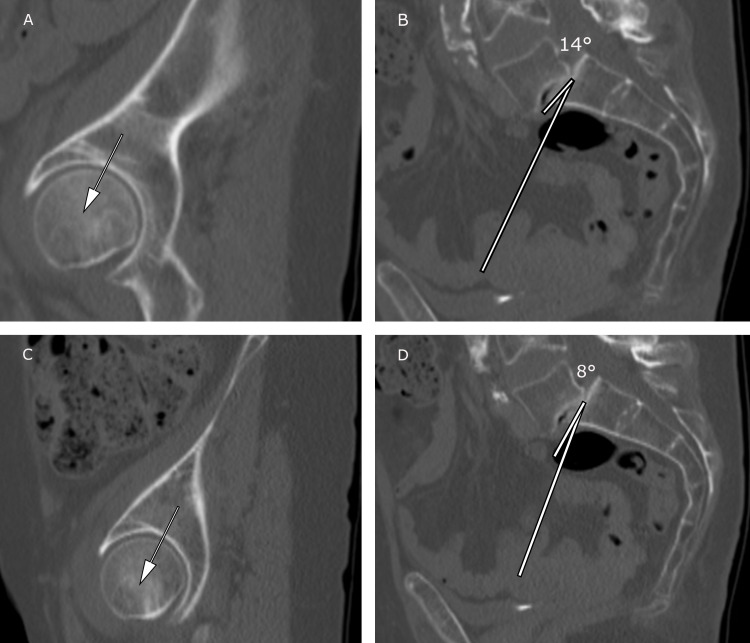
Methods: A retrospective, cross-sectional study of PI in a consecutive cohort of patients' pelvic/abdominal CT scans from an emergency room visit at a Level 1 trauma center between 2013 and 2016. Inclusion criteria was >18 years and had no lumbar or pelvis fracture. A total of 361 patients met the criteria for our study. We documented age, average PI, and SPL (type, grading, and location). Sagittal CT scans were used to measure PI (between hip axis to an orthogonal line originating at the center of superior end plate axis of first sacral vertebra). Patients were categorized: with SPL (n=45) and without SPL (n=316). Subgroups were comprised based on the location of SPL (L4/L5 and L5/S1) and type of SPL. Analysis of variance (ANOVA) and chi-square tests used; p≤0.05 considered statistically significant.
Results: Patients with SPL were significantly older versus patients without SPL, p=0.006. There were no statistical differences in PI between patients with and without SPL (p=0.29); between subgroups of patients with SPL at L4/L5 and without SPL (p=0.52); between subgroups with type of SPL at L4/L5 and without SPL (p=0.47); and between SPL patients at L5/S1 and without SPL (p=0.40). Patients with isthmic SPL at L5/S1 had nearly significant higher PIs (p=0.06) compared to those without SPL or with degenerative SPL at L5/S1. There was a trend towards higher PI in Grade 2 SPL patients at L5/S1, p=0.18.
Conclusions: Patients with SPL were significantly older than patients without SPL. The two trends observed were that PI was higher in patients with isthmic SPL at L5/S1 and an increased PI with Grade 2 isthmic SPL at L5/S1. Our reported CT PI measurements correlated with reported PI measured using standard radiographs in patients with SPL. CT scans may be a reliable modality to evaluate adult SPL.
Keywords: age; computed tomography (ct); degenerative spondylolisthesis; isthmic spondylolisthesis; lumbar lordosis; pelvic incidence (pi); pelvic tilt; sacral slope; spinopelvic parameters; spondylolisthesis.
Copyright © 2022, Shi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Spondylolysis: a review and reappraisal. Syrmou E, Tsitsopoulos PP, Marinopoulos D, Tsonidis C, Anagnostopoulos I, Tsitsopoulos PD. https://www.ncbi.nlm.nih.gov. Hippokratia. 2010;14:17–21. - PMC - PubMed
-
- Impact of spinopelvic alignment on decision making in deformity surgery in adults: a review. Ames CP, Smith JS, Scheer JK, et al. J Neurosurg Spine. 2012;16:547–564. - PubMed
-
- Sagittal plane considerations and the pelvis in the adult patient. Schwab F, Lafage V, Patel A, Farcy JP. Spine (Phila Pa 1976) 2009;34:1828–1833. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous