

A new approach for the acquisition of trauma surgical skills: an OSCE type of simulation training program
- PMID: 35237901
- PMCID: PMC8890468
- DOI: 10.1007/s00464-022-09098-w
A new approach for the acquisition of trauma surgical skills: an OSCE type of simulation training program
Abstract
Background: Worldwide, trauma-related deaths are one of the main causes of mortality. Appropriate surgical treatment is crucial to prevent mortality, however, in the past decade, general surgery residents' exposure to trauma cases has decreased, particularly since the COVID-19 pandemic. In this context, accessible simulation-based training scenarios are essential.
Methods: A low-cost, previously tested OSCE scenario for the evaluation of surgical skills in trauma was implemented as part of a short training boot camp for residents and recently graduated surgeons. The following stations were included bowel anastomosis, vascular anastomosis, penetrating lung injury, penetrating cardiac injury, and gastric perforation (laparoscopic suturing). A total of 75 participants from 15 different programs were recruited. Each station was videotaped in high definition and assessed in a remote and asynchronous manner. The level of competency was assessed through global and specific rating scales alongside procedural times. Self-confidence to perform the procedure as the leading surgeon was evaluated before and after training.
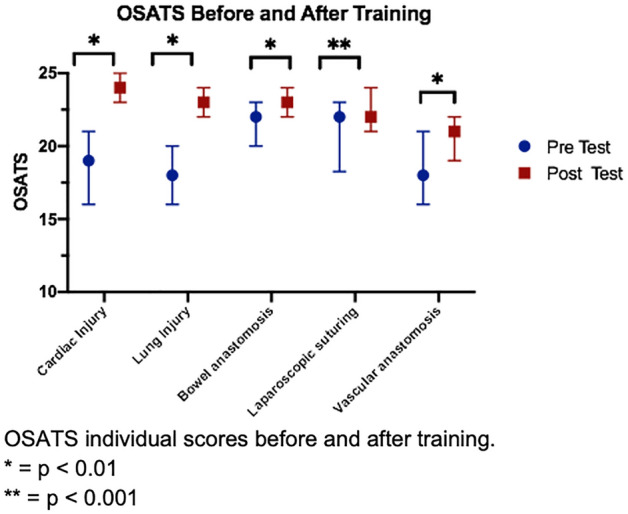
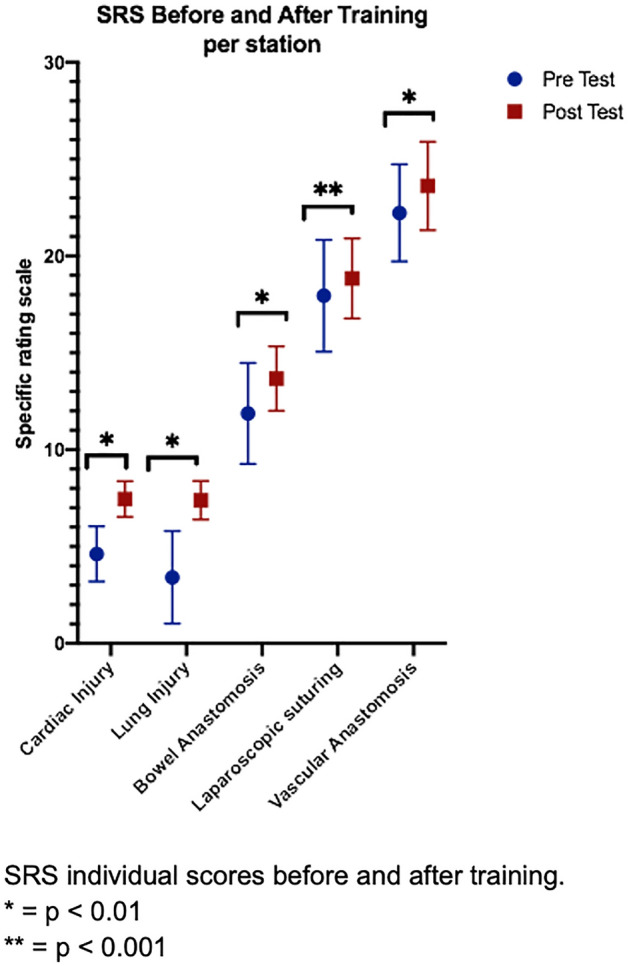
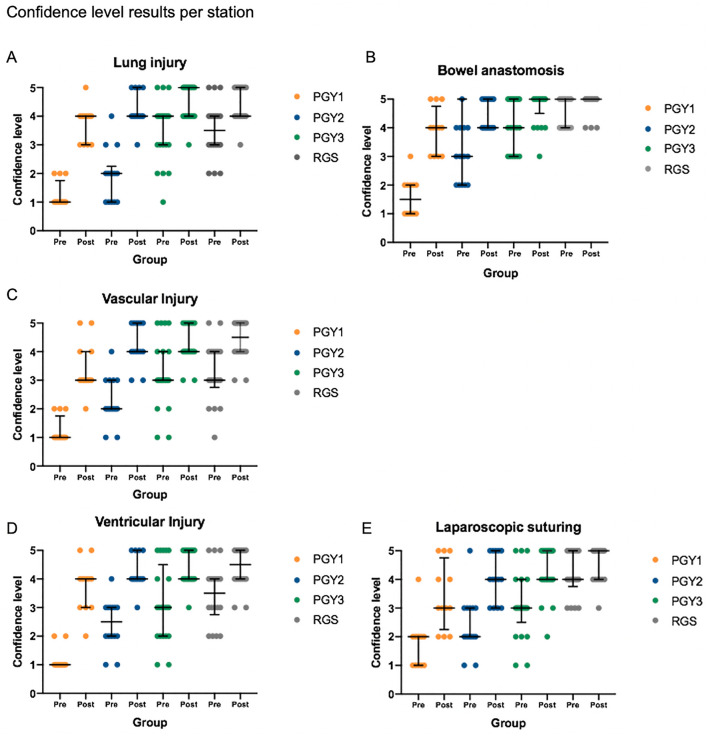
Results: Statistically significant differences were found in pre-training scores between groups for all stations. The lowest scores were obtained in the cardiac and lung injury stations. After training, participants significantly increased their level of competence in both grading systems. Procedural times for the pulmonary tractotomy, bowel anastomosis, and vascular anastomosis stations increased after training. A significant improvement in self-confidence was shown in all stations.
Conclusion: An OSCE scenario for training surgical skills in trauma was effective in improving proficiency level and self-confidence. Low pre-training scores and level of confidence in the cardiac and lung injury stations represent a deficit in residency programs that should be addressed. The incorporation of simulation-based teaching tools at early stages in residency would be beneficial when future surgeons face extremely severe trauma scenarios.
Keywords: Simulation training; Surgical education technology; Surgical training; Trauma surgery.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Drs. Catalina Ortiz, Javier Vela, Caterina Contreras, Francisca Belmar, Ivan Paul, Analia Zinco, Juan Pablo Ramos, Pablo Ottolino, Pablo Achurra, Nicolas Jarufe, and Julian Varas were financed and supported by a Chilean Research Grant FONDECYT REG 1171908 from CONICYT and by the Department of Digestive Surgery, Faculty of Medicine, Pontificia Universidad Católica de Chile. Dr. Julian Varas is the Founder of Training Competence, an official spinoff startup from the Pontificia Universidad Católica de Chile. The startup and the Pontificia Universidad Católica de Chile are the owners of the rights and distribution of the C1DO1 platform used for the assessment in this study. Dr. Adnan Alseidi has no conflict of interest or financial ties to disclose.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
