

Comparison of Strategies for Typhoid Conjugate Vaccine Introduction in India: A Cost-Effectiveness Modeling Study
- PMID: 35238367
- PMCID: PMC8892534
- DOI: 10.1093/infdis/jiab150
Comparison of Strategies for Typhoid Conjugate Vaccine Introduction in India: A Cost-Effectiveness Modeling Study
Abstract
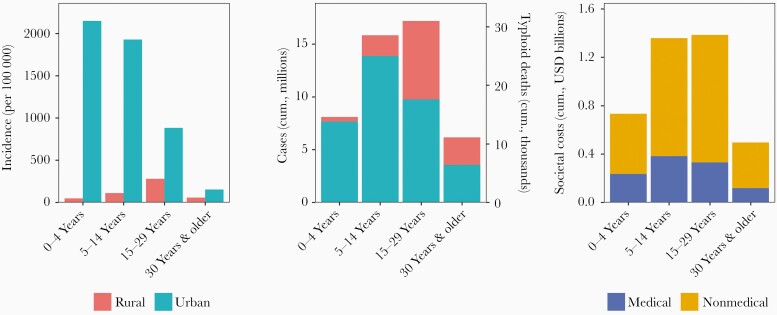
Background: Typhoid fever causes substantial global mortality, with almost half occurring in India. New typhoid vaccines are highly effective and recommended by the World Health Organization for high-burden settings. There is a need to determine whether and which typhoid vaccine strategies should be implemented in India.
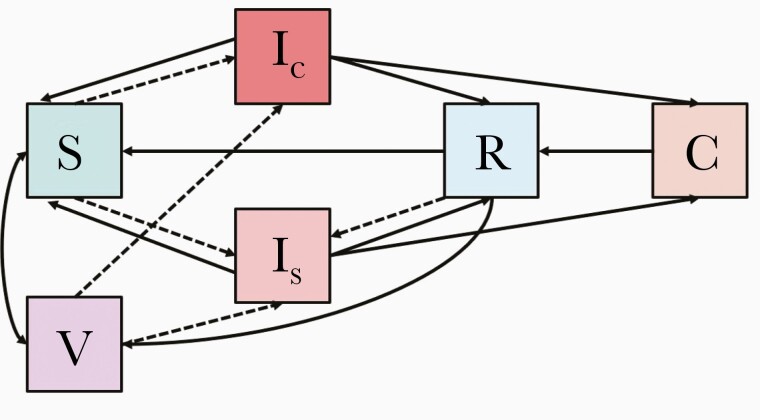
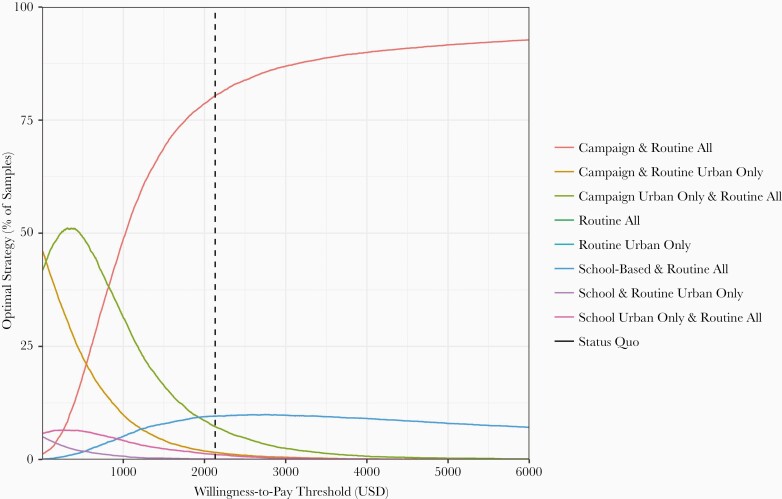
Methods: We assessed typhoid vaccination using a dynamic compartmental model, parameterized by and calibrated to disease and costing data from a recent multisite surveillance study in India. We modeled routine and 1-time campaign strategies that target different ages and settings. The primary outcome was cost-effectiveness, measured by incremental cost-effectiveness ratios (ICERs) benchmarked against India's gross national income per capita (US$2130).
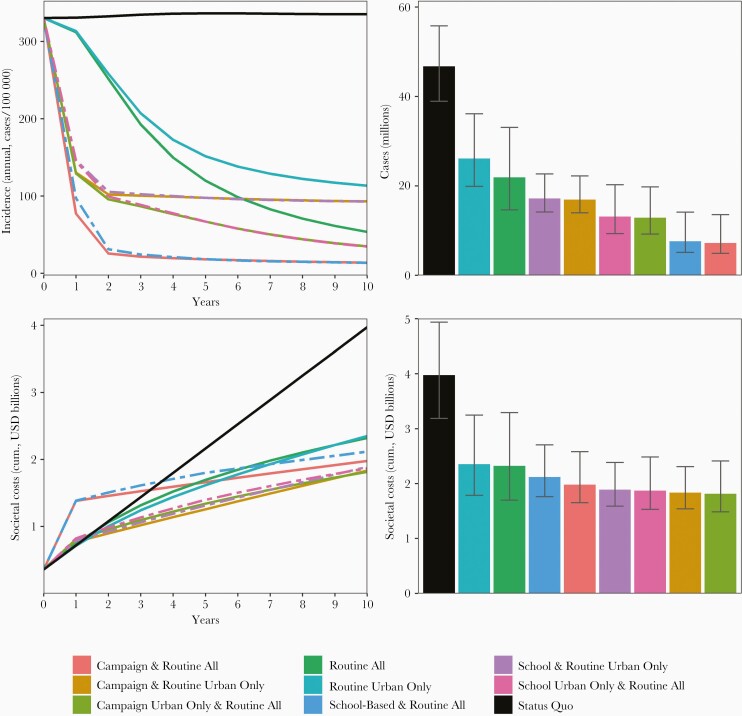
Results: Both routine and campaign vaccination strategies were cost-saving compared to the status quo, due to averted costs of illness. The preferred strategy was a nationwide community-based catchup campaign targeting children aged 1-15 years alongside routine vaccination, with an ICER of $929 per disability-adjusted life-year averted. Over the first 10 years of implementation, vaccination could avert 21-39 million cases and save $1.6-$2.2 billion. These findings were broadly consistent across willingness-to-pay thresholds, epidemiologic settings, and model input distributions.
Conclusions: Despite high initial costs, routine and campaign typhoid vaccination in India could substantially reduce mortality and was highly cost-effective.
Keywords: India; cost-effectiveness; enteric fever; model; typhoid; vaccines.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
