

Editorial
doi: 10.1165/rcmb.2021-0549ED.
Targeting ATP-Sensitive K+ Channels to Treat Pulmonary Hypertension
Affiliations
- PMID: 35238728
- PMCID: PMC9116352
- DOI: 10.1165/rcmb.2021-0549ED
Item in Clipboard
Editorial
Targeting ATP-Sensitive K+ Channels to Treat Pulmonary Hypertension
Am J Respir Cell Mol Biol.
2022 May.
No abstract available
Figures
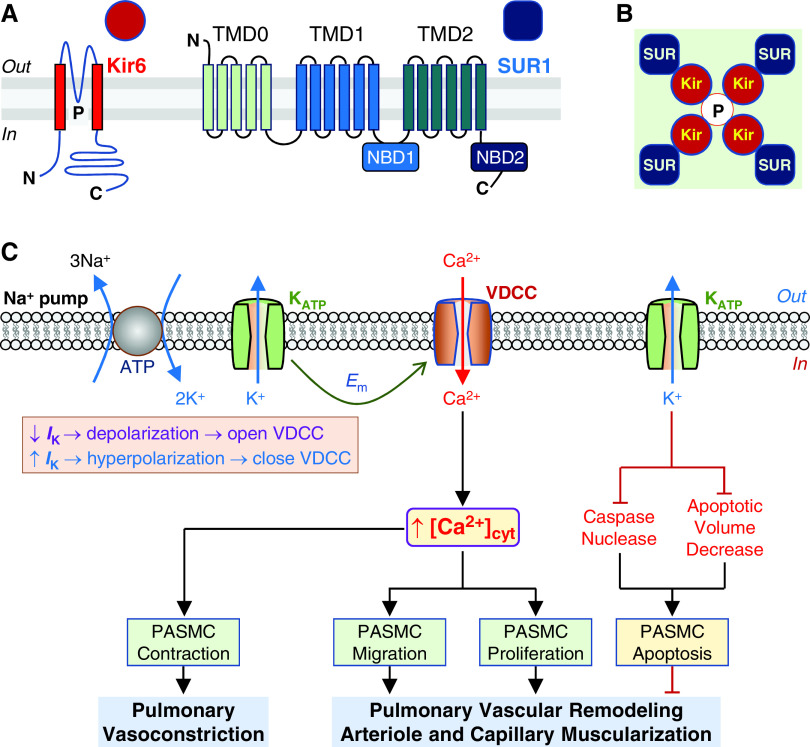
Structure of ATP-sensitive K+ (KATP) channel and potential therapeutic role of KATP channel activators in pulmonary hypertension (PH). KATP channel, which is inhibited by intracellular ATP, is formed by the inward-rectifier K+ (Kir6.1 or Kir6.2) channel subunit and the sulfonylurea receptor (SUR1 or SUR2) subunit. (A and B) Topology of the Kir6 and SUR1 (A) and the KATP channel formed by Kir6 tetrameric core (red circles and the pore, P) and four peripheral SUR1 subunits (blue squares) (B). The Kir6 monomer contains two transmembrane spans with the pore region (P) located between the two transmembrane helices, and both N- and C-termini are in the intracellular site. SUR1 contains three transmembrane domains (TMD), TMD0 (with five transmembrane α-helices), TMD1 (with six transmembrane α-helices), and TMD2 (with six transmembrane α-helices). TMD0 is connected by a long cytosolic loop known as the CL3 linker. There are two nucleotide-binding domains (NBDs), NBD1 (located at the cytosolic loop between TMD1 and TMD2) and NBD2 (at the C-terminus) of TMD2. (C) Proposed mechanisms involved in the therapeutic effect of KATP channel activation on pulmonary vasoconstriction and vascular remodeling, the major causes for the elevated pulmonary vascular resistance (PVR) and pulmonary arterial pressure (PAP) in patients with PAH/PH. Membrane potential (Em) in pulmonary artery smooth muscle cells (PASMCs) is regulated by the activity of electrogenic Na+ pump and K+ channels in the plasma membrane. Decreased (↓) K+ currents (IK) due to inhibited KATP channel activity and/or downregulated Kir6/SUR1 expression result in membrane depolarization that subsequently opens voltage-dependent Ca2+ channels (VDCC), enhances Ca2+ influx through VDCC, and increases cytosolic Ca2+ concentration ([Ca2+]cyt) in PASMCs. A rise in [Ca2+]cyt causes PASMC contraction and thus pulmonary vasoconstriction and stimulates PASMC migration and proliferation that contributes to the development and progression of concentric pulmonary vascular remodeling and muscularization of pulmonary arteriole and capillary. Increased (↑) IK as a result, for example, of activation of KATP channels by cromakalim and diazoxide, causes membrane hyperpolarization or repolarization that subsequently closes VDCC. The resultant inhibition of Ca2+ influx through VDCC and decreases in [Ca2+]cyt lead to pulmonary vasodilation and regression of remodeled pulmonary arteries and arterioles. Furthermore, activation of K+ efflux through KATP channels (and other types of K+ channels) would relieve K+-mediated inhibition of caspase and nuclease activity and enhance PASMC apoptosis. Activation of K+ efflux through KATP channels would also facilitate apoptotic volume decrease, an early hallmark of apoptosis, and induce PASMC apoptosis. The inhibitory effects of KATP channel activation (via Kir6 and/or SUR1) on pulmonary vasoconstriction and vascular remodeling and the apoptotic effect on highly proliferated cells in the remodeled distal arteries all contribute to the potential therapeutic effects of the KATP channel activators.
Comment on
-
SUR1 As a New Therapeutic Target for Pulmonary Arterial Hypertension.Am J Respir Cell Mol Biol. 2022 May;66(5):539-554. doi: 10.1165/rcmb.2021-0180OC. Am J Respir Cell Mol Biol. 2022. PMID: 35175177
References
-
- Montani D, Chaumais MC, Guignabert C, Günther S, Girerd B, Jaïs X, et al. Targeted therapies in pulmonary arterial hypertension. Pharmacol Ther . 2014;141:172–191. - PubMed
-
- Le Ribeuz H, Masson B, Capuano V, Dutheil M, Gooroochurn H, Boët A, et al. SUR1 as a new therapeutic target for pulmonary arterial hypertension. Am J Respir Cell Mol Biol . 2022;66 - PubMed
-
- Papp R, Nagaraj C, Zabini D, Nagy BM, Lengyel M, Skofic Maurer D, et al. Targeting TMEM16A to reverse vasoconstriction and remodelling in idiopathic pulmonary arterial hypertension. Eur Respir J . 2019;53:1800965. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
