

Optimal effectiveness of heart failure management - an umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure
- PMID: 35239106
- PMCID: PMC8892116
- DOI: 10.1007/s10741-021-10212-8
Optimal effectiveness of heart failure management - an umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure
Abstract
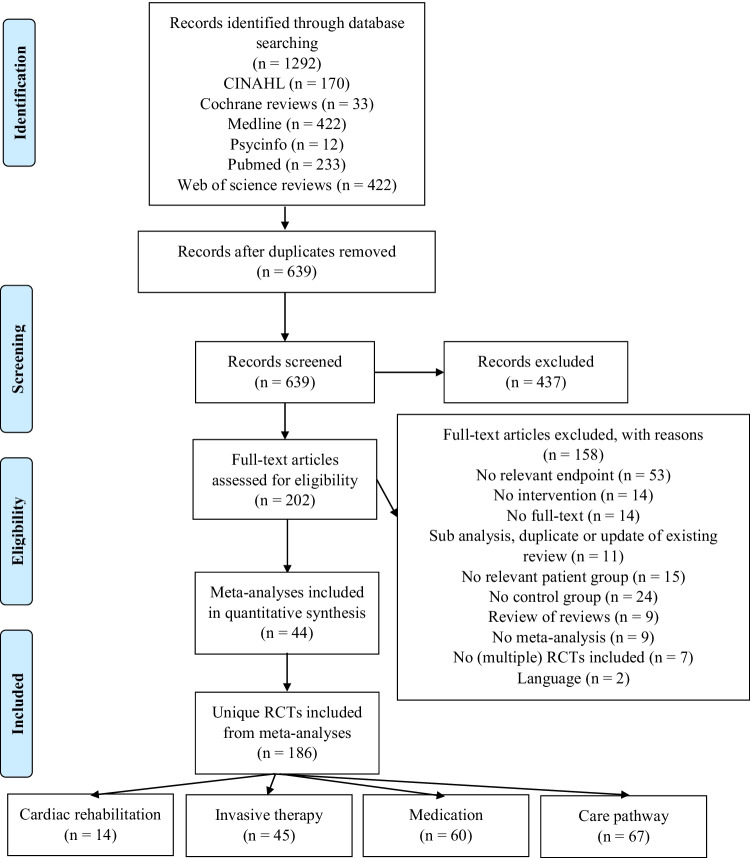
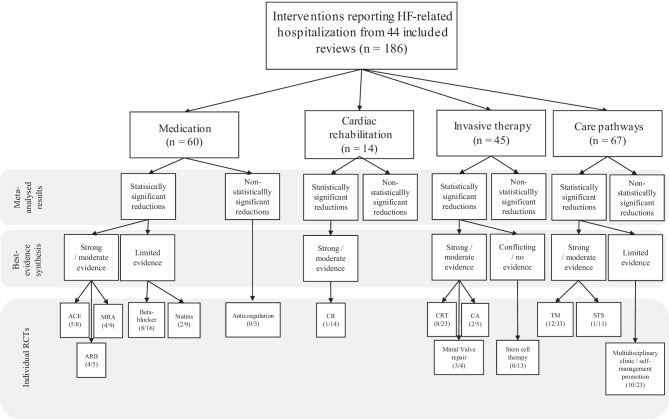
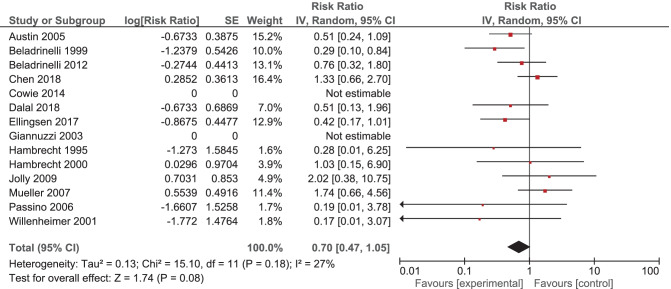
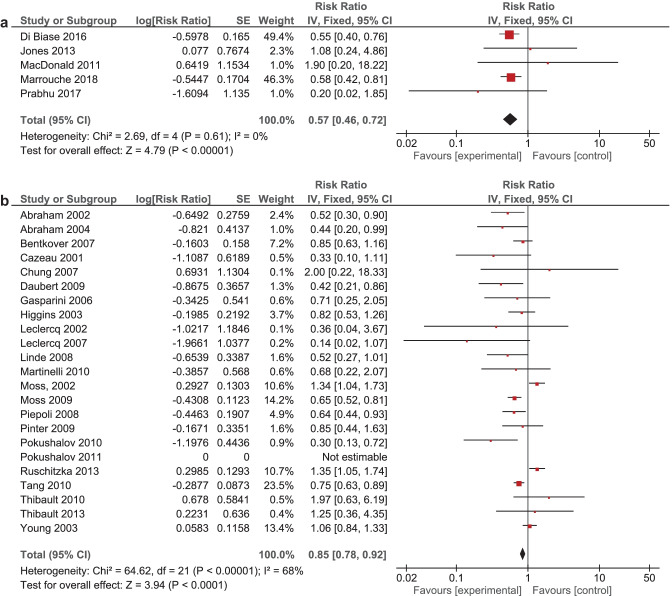
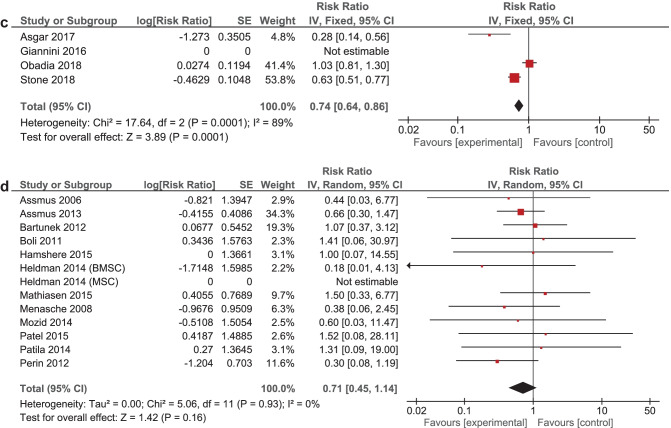
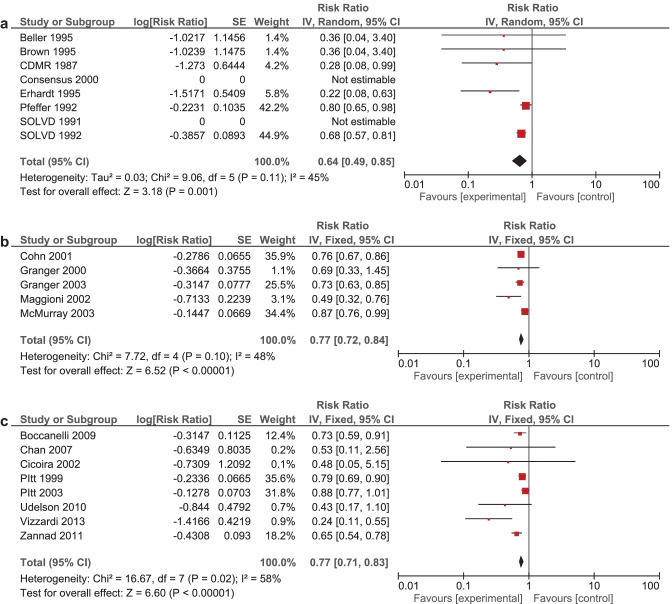
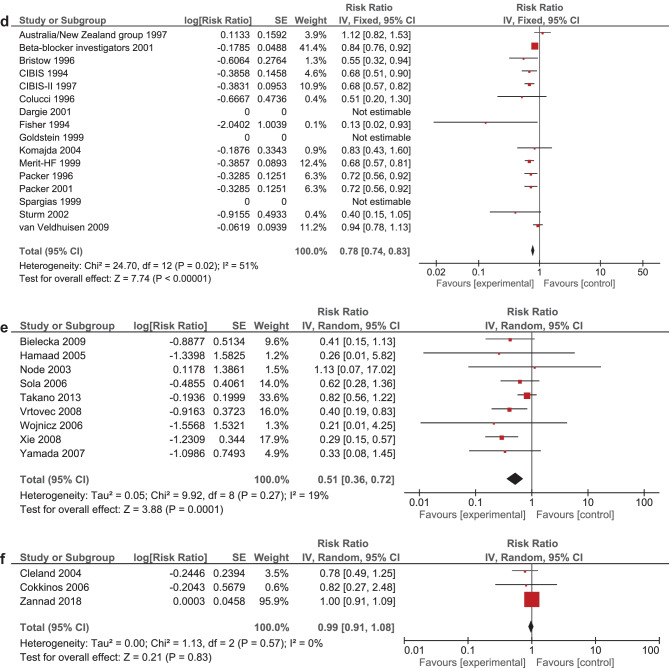
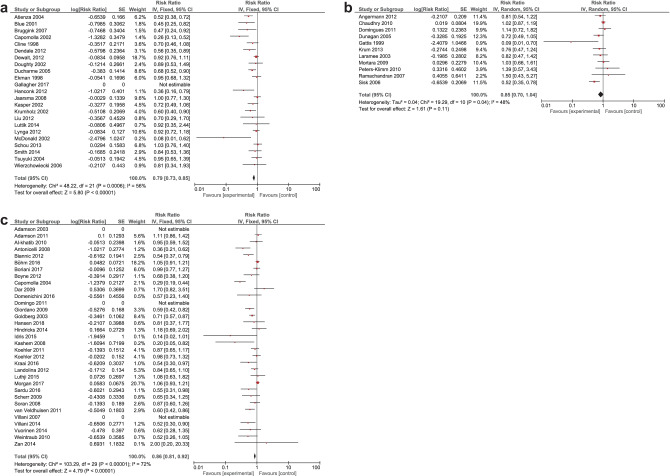
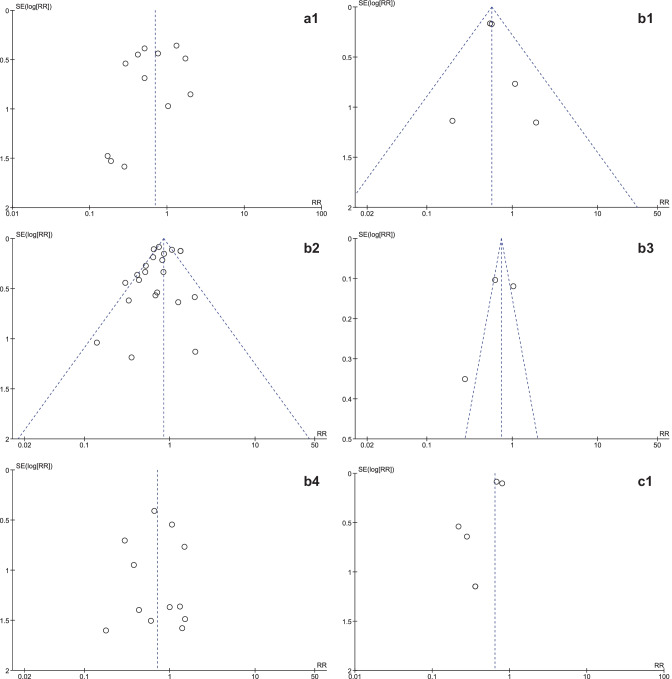
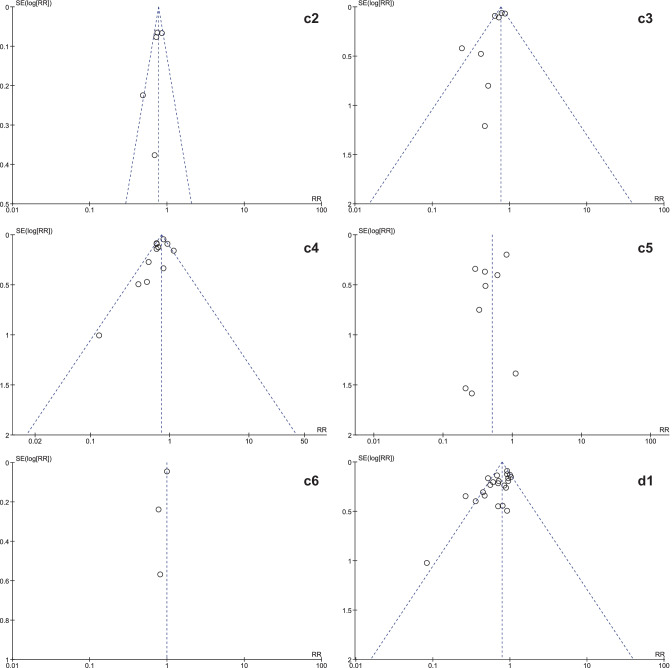
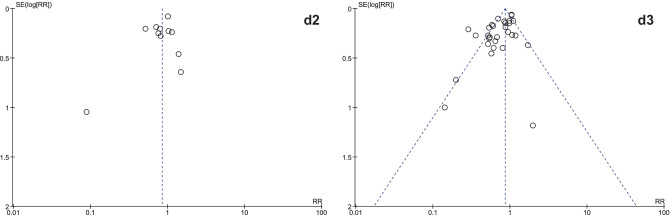
Heart failure (HF) is a major health concern, which accounts for 1-2% of all hospital admissions. Nevertheless, there remains a knowledge gap concerning which interventions contribute to effective prevention of HF (re)hospitalization. Therefore, this umbrella review aims to systematically review meta-analyses that examined the effectiveness of interventions in reducing HF-related (re)hospitalization in HFrEF patients. An electronic literature search was performed in PubMed, Web of Science, PsycInfo, Cochrane Reviews, CINAHL, and Medline to identify eligible studies published in the English language in the past 10 years. Primarily, to synthesize the meta-analyzed data, a best-evidence synthesis was used in which meta-analyses were classified based on level of validity. Secondarily, all unique RCTS were extracted from the meta-analyses and examined. A total of 44 meta-analyses were included which encompassed 186 unique RCTs. Strong or moderate evidence suggested that catheter ablation, cardiac resynchronization therapy, cardiac rehabilitation, telemonitoring, and RAAS inhibitors could reduce (re)hospitalization. Additionally, limited evidence suggested that multidisciplinary clinic or self-management promotion programs, beta-blockers, statins, and mitral valve therapy could reduce HF hospitalization. No, or conflicting evidence was found for the effects of cell therapy or anticoagulation. This umbrella review highlights different levels of evidence regarding the effectiveness of several interventions in reducing HF-related (re)hospitalization in HFrEF patients. It could guide future guideline development in optimizing care pathways for heart failure patients.
Keywords: Care pathways; Heart failure related hospitalizations; Interventions; Invasive therapy; Medication; Rehabilitations.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Community-based care for the specialized management of heart failure: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(17):1-42. Epub 2009 Nov 1. Ont Health Technol Assess Ser. 2009. PMID: 23074521 Free PMC article.
-
Disease management interventions for heart failure.Cochrane Database Syst Rev. 2019 Jan 8;1(1):CD002752. doi: 10.1002/14651858.CD002752.pub4. Cochrane Database Syst Rev. 2019. PMID: 30620776 Free PMC article.
-
No benefits of statins for sudden cardiac death prevention in patients with heart failure and reduced ejection fraction: A meta-analysis of randomized controlled trials.PLoS One. 2017 Feb 6;12(2):e0171168. doi: 10.1371/journal.pone.0171168. eCollection 2017. PLoS One. 2017. PMID: 28166237 Free PMC article.
-
Behavioural interventions for type 2 diabetes: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(21):1-45. Epub 2009 Oct 1. Ont Health Technol Assess Ser. 2009. PMID: 23074526 Free PMC article.
-
Effectiveness of telemedicine systems for adults with heart failure: a meta-analysis of randomized controlled trials.Heart Fail Rev. 2020 Mar;25(2):231-243. doi: 10.1007/s10741-019-09801-5. Heart Fail Rev. 2020. PMID: 31197564 Free PMC article. Review.
Cited by
-
RELEASE-HF study: a protocol for an observational, registry-based study on the effectiveness of telemedicine in heart failure in the Netherlands.BMJ Open. 2024 Jan 4;14(1):e078021. doi: 10.1136/bmjopen-2023-078021. BMJ Open. 2024. PMID: 38176879 Free PMC article.
-
Treatment outcomes and associated factors among chronic ambulatory heart failure patients at Jimma Medical Center, South West Ethiopia: prospective observational study.BMC Cardiovasc Disord. 2023 Jan 17;23(1):26. doi: 10.1186/s12872-023-03055-8. BMC Cardiovasc Disord. 2023. PMID: 36650423 Free PMC article.
-
Alternatives to Hospitalization: Adding the Patient Voice to Advanced Heart Failure Management.CJC Open. 2023 Apr 5;5(6):454-462. doi: 10.1016/j.cjco.2023.03.014. eCollection 2023 Jun. CJC Open. 2023. PMID: 37397619 Free PMC article. Review.
-
Historical Gaps in the Integration of Patient-Centric Self-Management Components in HFrEF Interventions: An Umbrella Narrative Review.J Clin Med. 2025 Apr 19;14(8):2832. doi: 10.3390/jcm14082832. J Clin Med. 2025. PMID: 40283663 Free PMC article. Review.
-
Randomized Controlled Trial Comparing a Multidisciplinary Intervention by a Geriatrician and a Cardiologist to Usual Care after a Heart Failure Hospitalization in Older Patients: The SENECOR Study.J Clin Med. 2022 Mar 30;11(7):1932. doi: 10.3390/jcm11071932. J Clin Med. 2022. PMID: 35407540 Free PMC article.
References
-
- Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Vartiainen E, Sans S, Pasterkamp G, Hughes M, Costanzo S, Donati MB, Jousilahti P, Linneberg A, Palosaari T, de Gaetano G, Bobak M, den Ruijter HM, Jørgensen T, Söderberg S, Kuulasmaa K, Zeller T, Iacoviello L, Salomaa V, Schnabel RB. Sex-specific epidemiology of heart failure risk and mortality in Europe: results from the BiomarCaRE consortium. JACC Hear Fail. 2019;7:204–213. doi: 10.1016/j.jchf.2018.08.008. - DOI - PubMed
-
- Mamas MA, Sperrin M, Watson MC, Coutts A, Wilde K, Burton C, Kadam UT, Kwok CS, Clark AB, Murchie P. Do patients have worse outcomes in heart failure than in cancer? a primary care-based cohort study with 10-year follow-up in Scotland. Eur J Heart Fail Wiley Online Library. 2017;19:1095–1104. doi: 10.1002/ejhf.822. - DOI - PubMed
-
- Data from the American Heart Association (2000) Heart and stroke statistical update. Am Hear Assoc Dallas. TX
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
