

Social Determinants of Cardiovascular Disease
- PMID: 35239404
- PMCID: PMC8893132
- DOI: 10.1161/CIRCRESAHA.121.319811
Social Determinants of Cardiovascular Disease
Abstract
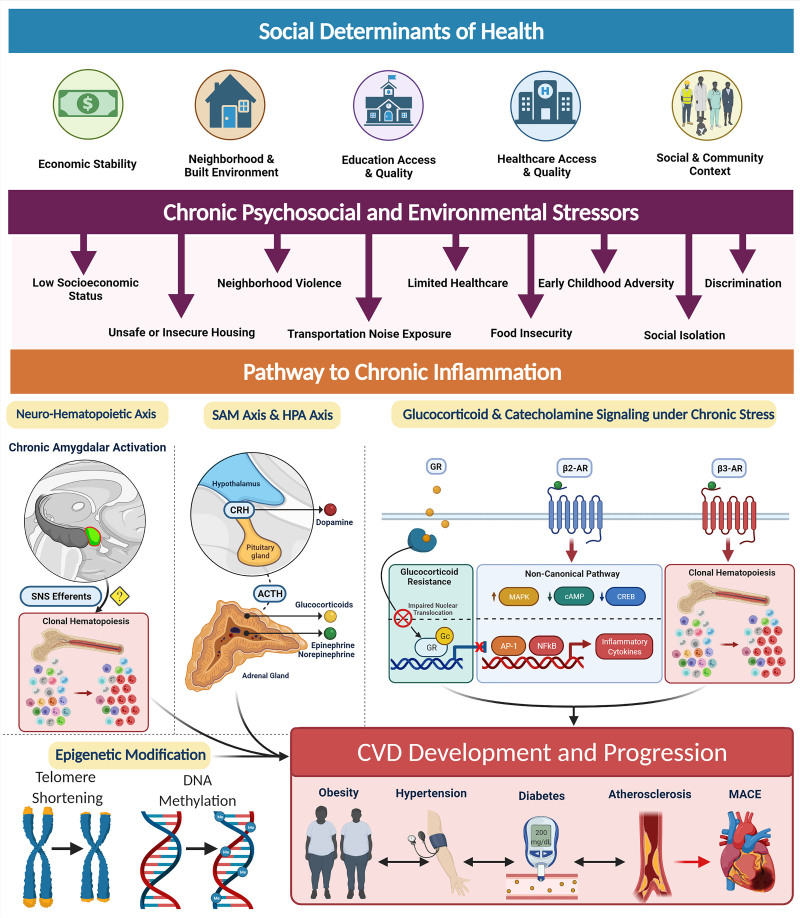
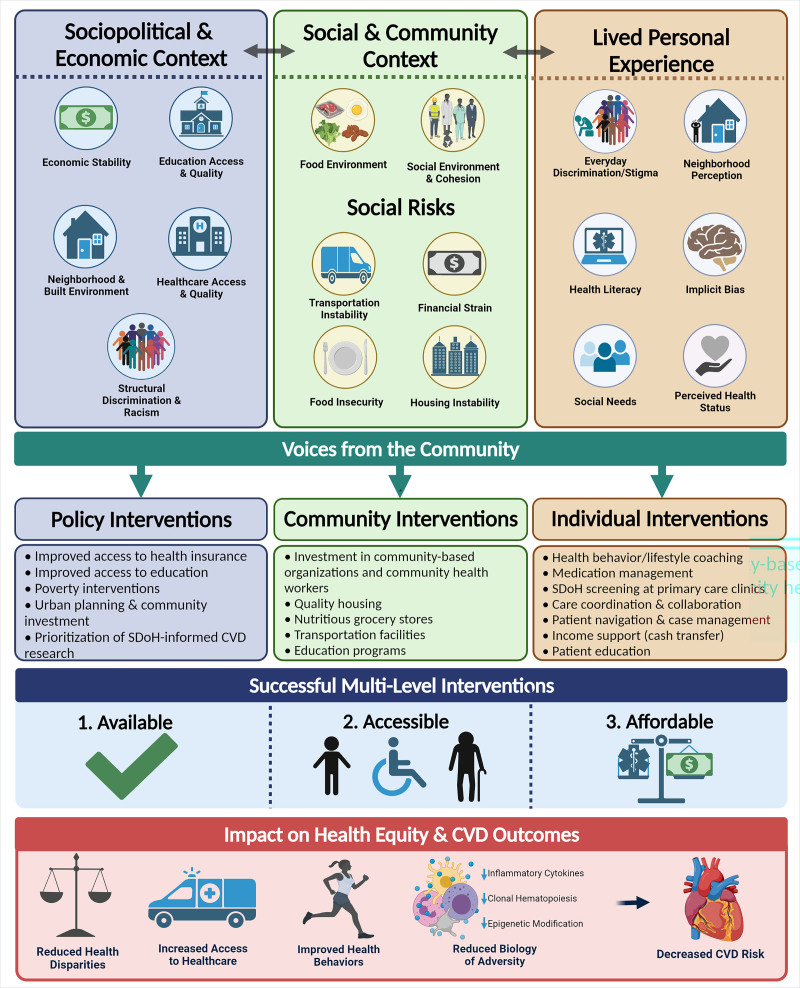
Social determinants of health (SDoH), which encompass the economic, social, environmental, and psychosocial factors that influence health, play a significant role in the development of cardiovascular disease (CVD) risk factors as well as CVD morbidity and mortality. The COVID-19 pandemic and the current social justice movement sparked by the death of George Floyd have laid bare long-existing health inequities in our society driven by SDoH. Despite a recent focus on these structural drivers of health disparities, the impact of SDoH on cardiovascular health and CVD outcomes remains understudied and incompletely understood. To further investigate the mechanisms connecting SDoH and CVD, and ultimately design targeted and effective interventions, it is important to foster interdisciplinary efforts that incorporate translational, epidemiological, and clinical research in examining SDoH-CVD relationships. This review aims to facilitate research coordination and intervention development by providing an evidence-based framework for SDoH rooted in the lived experiences of marginalized populations. Our framework highlights critical structural/socioeconomic, environmental, and psychosocial factors most strongly associated with CVD and explores several of the underlying biologic mechanisms connecting SDoH to CVD pathogenesis, including excess stress hormones, inflammation, immune cell function, and cellular aging. We present landmark studies and recent findings about SDoH in our framework, with careful consideration of the constructs and measures utilized. Finally, we provide a roadmap for future SDoH research focused on individual, clinical, and policy approaches directed towards developing multilevel community-engaged interventions to promote cardiovascular health.
Keywords: cardiovascular diseases; health status disparities; social determinants of health; social justice; socioeconomic factors.
Figures

References
-
- Becker T, Majmundar M, Harris K, eds. In: High and Rising Mortality Rates Among Working-Age Adults. Committee on Population, & National Academies of Sciences, Engineering, and Medicine. 2021. National Academies Press (US) - PubMed
-
- Harris KM, Woolf SH, Gaskin DJ. High and rising working-age mortality in the US: a report From the National Academies of Sciences, Engineering, and Medicine. JAMA. 2021;325:2045–2046. doi: 10.1001/jama.2021.4073 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
