

Driveline Infection in Left Ventricular Assist Device Patients: Effect of Standardized Protocols, Pathogen Type, and Treatment Strategy
- PMID: 35239537
- PMCID: PMC9469917
- DOI: 10.1097/MAT.0000000000001690
Driveline Infection in Left Ventricular Assist Device Patients: Effect of Standardized Protocols, Pathogen Type, and Treatment Strategy
Abstract
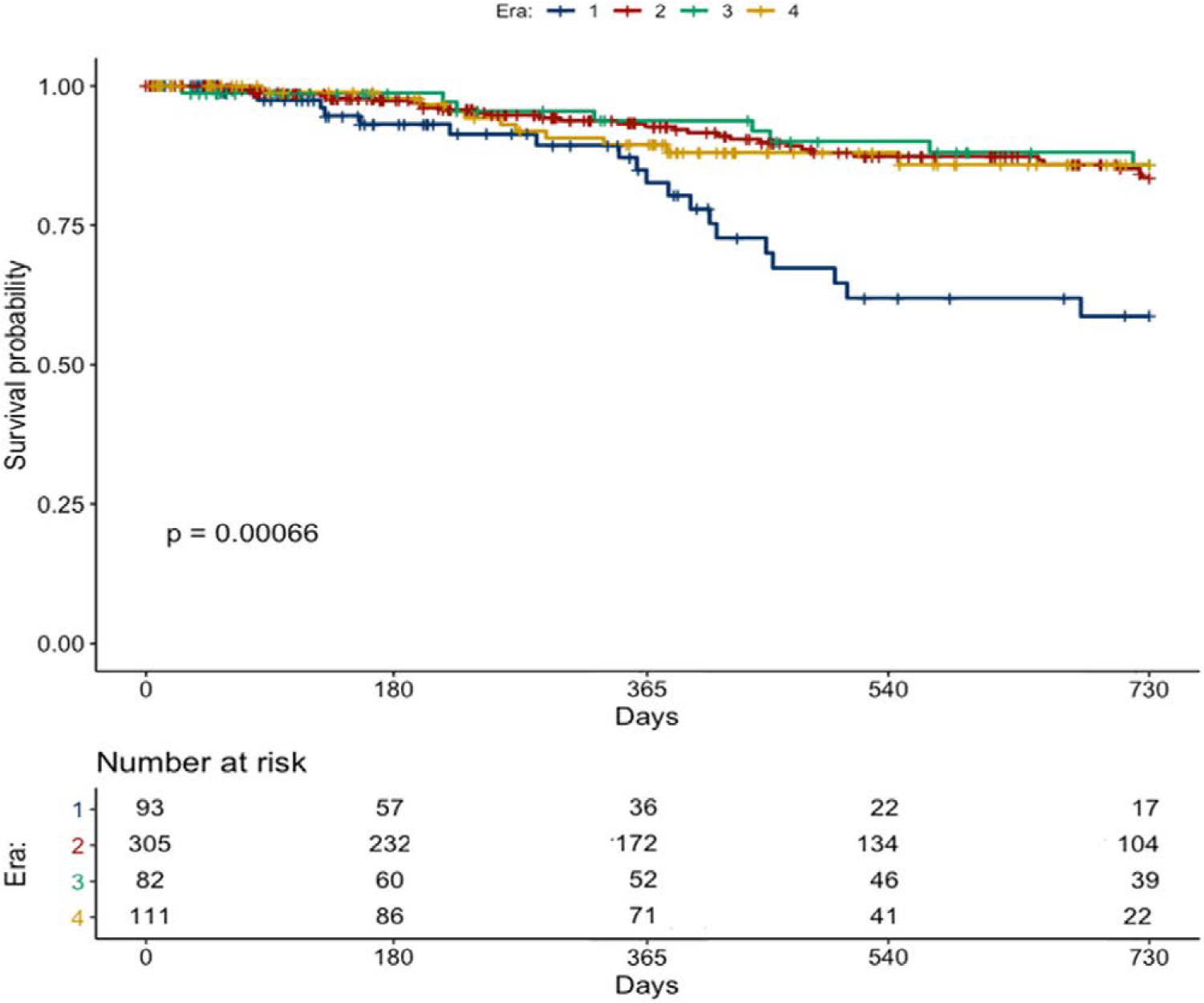
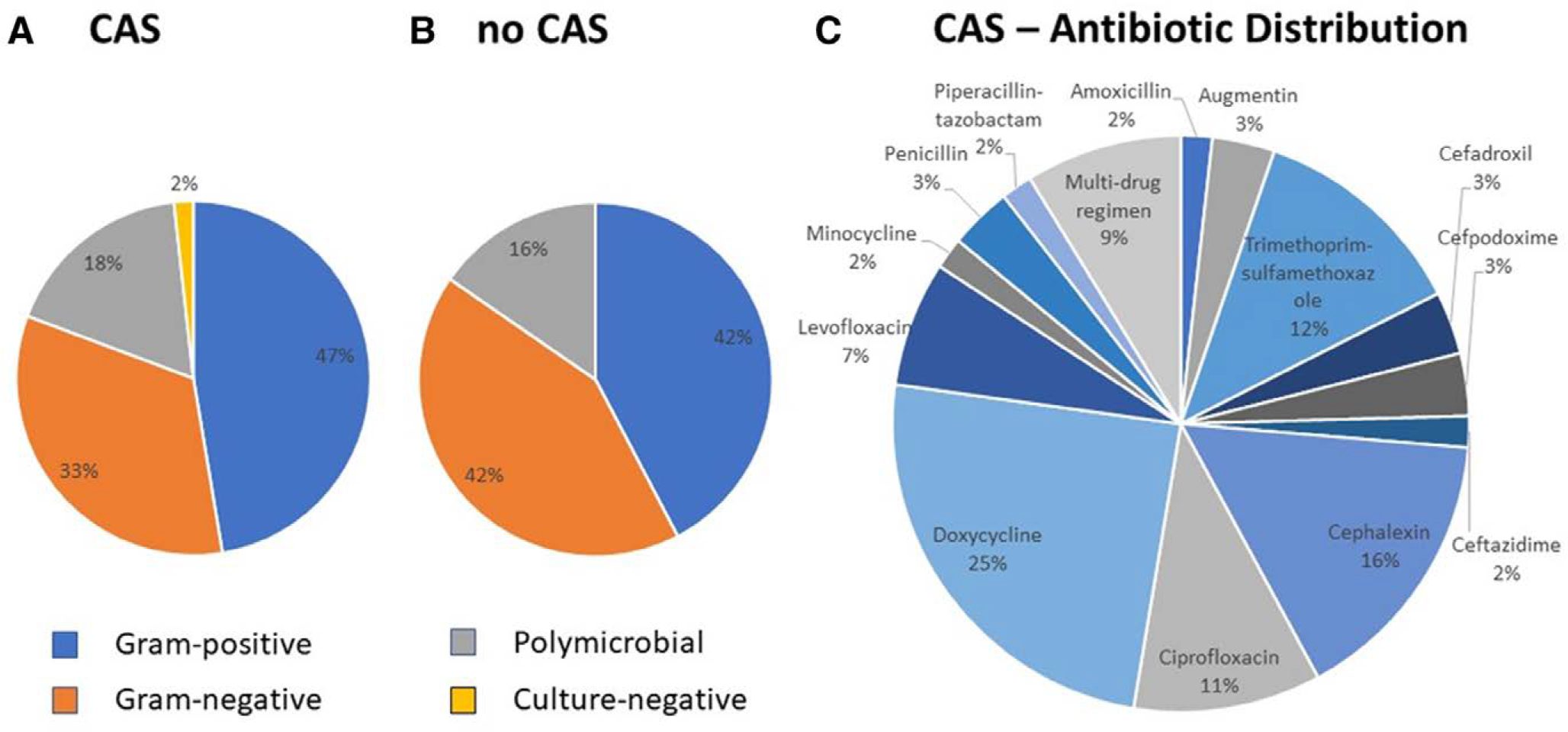
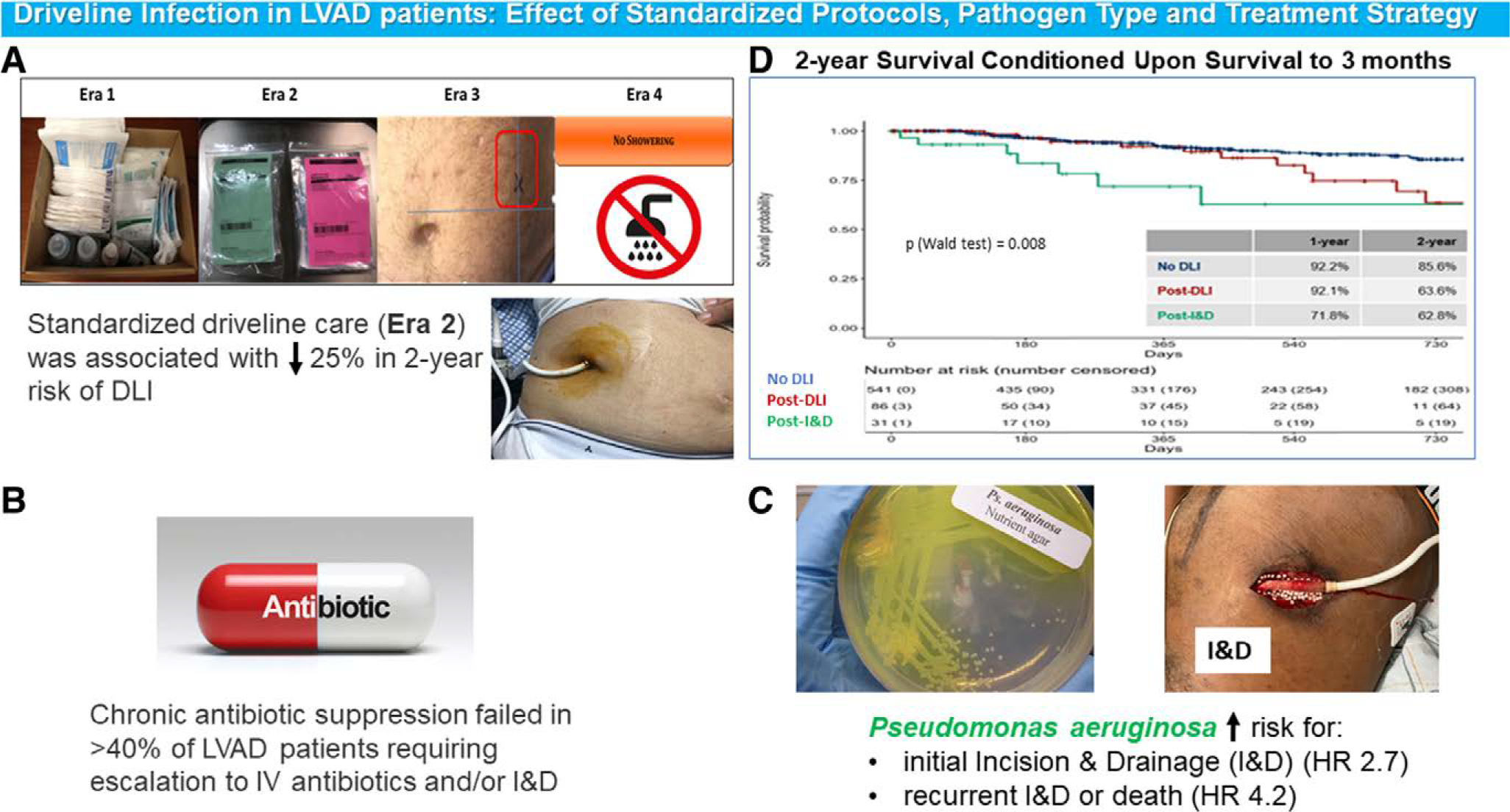
Driveline infection (DLI) is common after left ventricular assist device (LVAD). Limited data exist on DLI prevention and management. We investigated the impact of standardized driveline care initiatives, specific pathogens, and chronic antibiotic suppression (CAS) on DLI outcomes. 591 LVAD patients were retrospectively categorized based on driveline care initiatives implemented at our institution (2009-2019). Era (E)1: nonstandardized care; E2: standardized driveline care protocol; E3: addition of marking driveline exit site; E4: addition of "no shower" policy. 87(15%) patients developed DLI at a median (IQR) of 403(520) days. S. aureus and P. aeruginosa were the most common pathogens. 31 (36%) of DLI patients required incision and drainage (I&D) and 5 (5.7%) device exchange. P. aeruginosa significantly increased risk for initial I&D (HR 2.7, 95% CI, 1.1-6.3) and recurrent I&D or death (HR 4.2, 95% CI, 1.4-12.5). Initial I&D was associated with a significant increased risk of death (HR 2.92 (1.33-6.44); P = 0.008) when compared to patients who did not develop DLI. Implementation of standardized driveline care protocol (E2) was associated with increased 2-year freedom from DLI compared to nonstandardized care (HR 0.36, 95% CI, 0.2-0.6, P < 0.01). Additional preventive strategies (E3&E4) showed no further reduction in DLI rates. 57(65%) DLI patients received CAS, 44% of them required escalation to intravenous antibiotics and/or I&D. Presence of P. aeruginosa DLI markedly increased risk for I&D or death. Conditional survival of patients progressing to I&D is diminished. Standardized driveline care protocol was associated with a significant reduction in DLI, while additional preventive strategies require further testing.
Copyright © ASAIO 2022.
Conflict of interest statement
Disclosure: P.C.C. is recipient of a research grant from Abbott; he also serves as a consultant for the same company. Y.N. serves as a consultant for Abbott, CryoLife, and Zimmer-Biomet, and as a speaker for Nipro Co. G.T.S. serves as a consultant for Abbott. N.U. serves on advisory boards for Leviticus and Livemetric/Cormetric; he also serves as a consultant for Abbott and Medtronic. The remaining authors have no conflicts of interest to report.
Figures
Comment in
-
Driveline Infections Associated With Durable Left Ventricular Assist Device Support: An Ounce of Prevention is Worth a Pound of Cure.ASAIO J. 2022 Dec 1;68(12):1459-1460. doi: 10.1097/MAT.0000000000001857. Epub 2022 Nov 21. ASAIO J. 2022. PMID: 36410335 No abstract available.
References
-
- Teuteberg JJ, Cleveland JC Jr, Cowger J, et al.: The Society of Thoracic Surgeons Intermacs 2019 Annual Report: The Changing Landscape of Devices and Indications. Ann Thorac Surg 109: 649–660, 2020. - PubMed
-
- Quader MA, Wolfe LG, Kasirajan V: Heart transplantation outcomes in patients with continuous-flow left ventricular assist device-related complications. J Heart Lung Transplant 34: 75–81, 2015. - PubMed
-
- Kusne S, Mooney M, Danziger-Isakov L, et al.: An ISHLT consensus document for prevention and management strategies for mechanical circulatory support infection. J Heart Lung Transplant 36: 1137–1153, 2017. - PubMed
-
- Tattevin P, Flécher E, Auffret V, et al.: Risk factors and prognostic impact of left ventricular assist device-associated infections. Am Heart J 214: 69–76, 2019. - PubMed
-
- Pavlovic NV, Randell T, Madeira T, Hsu S, Zinoviev R, Abshire M: Risk of left ventricular assist device driveline infection: A systematic literature review. Heart Lung 48: 90–104, 2019. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
