

Ethnic inequalities in COVID-19 vaccine uptake and comparison to seasonal influenza vaccine uptake in Greater Manchester, UK: A cohort study
- PMID: 35239661
- PMCID: PMC8893324
- DOI: 10.1371/journal.pmed.1003932
Ethnic inequalities in COVID-19 vaccine uptake and comparison to seasonal influenza vaccine uptake in Greater Manchester, UK: A cohort study
Erratum in
-
Correction: Ethnic inequalities in COVID-19 vaccine uptake and comparison to seasonal influenza vaccine uptake in Greater Manchester, UK: A cohort study.PLoS Med. 2022 Apr 22;19(4):e1003982. doi: 10.1371/journal.pmed.1003982. eCollection 2022 Apr. PLoS Med. 2022. PMID: 35452447 Free PMC article.
Abstract
Background: COVID-19 vaccine uptake is lower amongst most minority ethnic groups compared to the White British group in England, despite higher COVID-19 mortality rates. Here, we add to existing evidence by estimating inequalities for 16 minority ethnic groups, examining ethnic inequalities within population subgroups, and comparing the magnitudes of ethnic inequalities in COVID-19 vaccine uptake to those for routine seasonal influenza vaccine uptake.
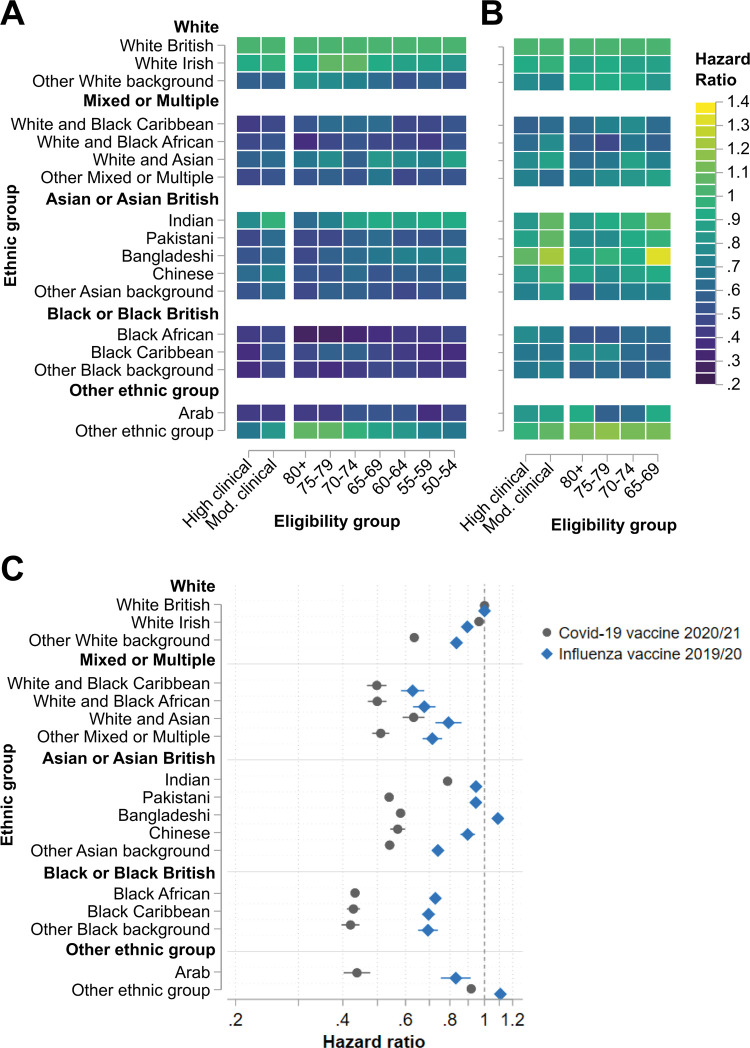
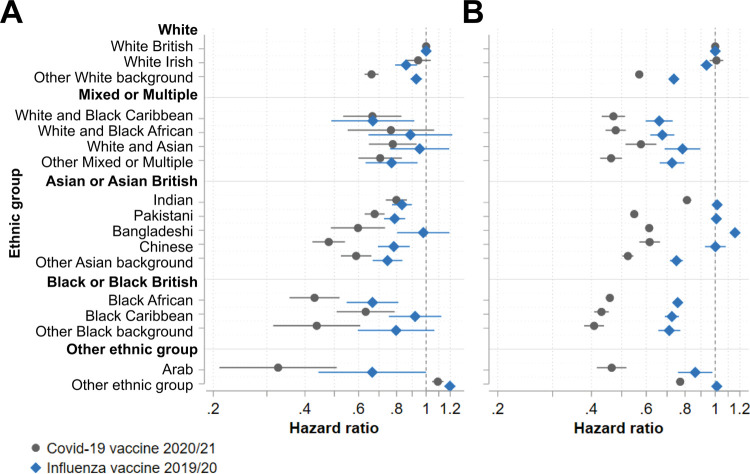
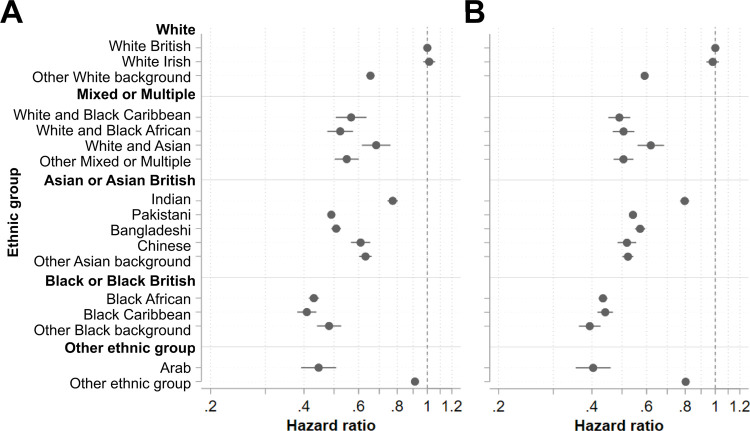
Methods and findings: We conducted a retrospective cohort study using the Greater Manchester Care Record, which contains de-identified electronic health record data for the population of Greater Manchester, England. We used Cox proportional hazards models to estimate ethnic inequalities in time to COVID-19 vaccination amongst people eligible for vaccination on health or age (50+ years) criteria between 1 December 2020 and 18 April 2021 (138 days of follow-up). We included vaccination with any approved COVID-19 vaccine, and analysed first-dose vaccination only. We compared inequalities between COVID-19 and influenza vaccine uptake adjusting by age group and clinical risk, and used subgroup analysis to identify populations where inequalities were widest. The majority of individuals (871,231; 79.24%) were White British. The largest minority ethnic groups were Pakistani (50,268; 4.75%), 'other White background' (43,195; 3.93%), 'other ethnic group' (34,568; 3.14%), and Black African (18,802; 1.71%). In total, 83.64% (919,636/1,099,503) of eligible individuals received a COVID-19 vaccine. Uptake was lower compared to the White British group for 15 of 16 minority ethnic groups, with particularly wide inequalities amongst the groups 'other Black background' (hazard ratio [HR] 0.42, 95% CI 0.40 to 0.44), Black African (HR 0.43, 95% CI 0.42 to 0.44), Arab (HR 0.43, 95% CI 0.40 to 0.48), and Black Caribbean (HR 0.43, 95% CI 0.42 to 0.45). In total, 55.71% (419,314/752,715) of eligible individuals took up influenza vaccination. Compared to the White British group, inequalities in influenza vaccine uptake were widest amongst the groups 'White and Black Caribbean' (HR 0.63, 95% CI 0.58 to 0.68) and 'White and Black African' (HR 0.67, 95% CI 0.63 to 0.72). In contrast, uptake was slightly higher than the White British group amongst the groups 'other ethnic group' (HR 1.11, 95% CI 1.09 to 1.12) and Bangladeshi (HR 1.08, 95% CI 1.05 to 1.11). Overall, ethnic inequalities in vaccine uptake were wider for COVID-19 than influenza vaccination for 15 of 16 minority ethnic groups. COVID-19 vaccine uptake inequalities also existed amongst individuals who previously took up influenza vaccination. Ethnic inequalities in COVID-19 vaccine uptake were concentrated amongst older and extremely clinically vulnerable adults, and the most income-deprived. A limitation of this study is the focus on uptake of the first dose of COVID-19 vaccination, rather than full COVID-19 vaccination.
Conclusions: Ethnic inequalities in COVID-19 vaccine uptake exceeded those for influenza vaccine uptake, existed amongst those recently vaccinated against influenza, and were widest amongst those with greatest COVID-19 risk. This suggests the COVID-19 vaccination programme has created additional and different inequalities beyond pre-existing health inequalities. We suggest that further research and policy action is needed to understand and remove barriers to vaccine uptake, and to build trust and confidence amongst minority ethnic communities.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: MS is an NIHR investigator. The other authors have declared no competing interests.
Figures
Comment in
-
Pre-existing health inequalities in vaccine uptake were exacerbated among ethnic communities during COVID-19 pandemic.Evid Based Nurs. 2023 Jan;26(1):22. doi: 10.1136/ebnurs-2022-103565. Epub 2022 Aug 11. Evid Based Nurs. 2023. PMID: 35953270 No abstract available.
References
-
- Public Health England. Disparities in the risk and outcomes of COVID19. London: Public Health England; 2020. [cited 2022 Feb 11]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploa....
-
- World Health Organization. Status of COVID-19 vaccines within WHO EUL/PQ evaluation process. Geneva: World Health Organization; 2021. [cited 2022 Feb 11]. Available from: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVI....
-
- Joint Committee on Vaccination and Immunisation. Joint Committee on Vaccination and Immunisation: advice on priority groups for COVID-19 vaccination, 30 December 2020. London: Joint Committee on Vaccination and Immunisation; 2021 [cited 2021 Mar 11]. Available from: https://www.gov.uk/government/publications/priority-groups-for-coronavir....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
