

Do Hungarian multiple sclerosis care units fulfil international criteria?
- PMID: 35239686
- PMCID: PMC8893632
- DOI: 10.1371/journal.pone.0264328
Do Hungarian multiple sclerosis care units fulfil international criteria?
Abstract
A patients: Because of the past 3 decades' extensive research, several disease modifying therapies became available, thus a paradigm change is multiple sclerosis care was necessary. In 2018 a therapeutic guideline was created recommending that treatment of persons with multiple sclerosis should take place in specified care units where the entire spectrum of disease modifying therapies is available, patient monitoring is ensured, and therapy side effects are detected and treated promptly. In 2019 multiple sclerosis care unit criteria were developed, emphasizing personnel and instrumental requirements to provide most professional care. However, no survey was conducted assessing the real-world adaptation of these criteria.
Objective: To assess whether Hungarian care units fulfil international criteria.
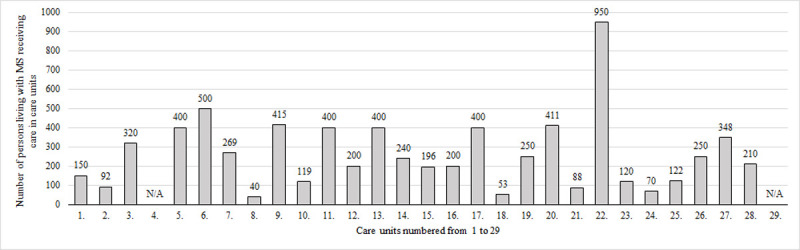
Methods: A self-report questionnaire was assembled based on international guidelines and sent to Hungarian care units focusing on 3 main aspects: personnel and instrumental background, disease-modifying therapy use, number of people living with multiple sclerosis receiving care in care units. Data on number of persons with multiple sclerosis were compared to Hungarian prevalence estimates. Descriptive statistics were used to analyse data.
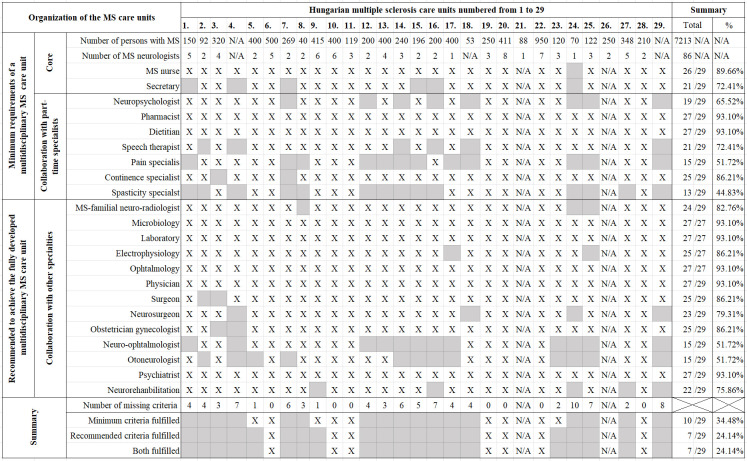
Results: Out of 27 respondent care units, 3 fulfilled minimum requirements and 7 fulfilled minimum and recommended requirements. The least prevalent neighbouring specialties were spasticity and pain specialist, and neuro-ophthalmologist and oto-neurologist. Only 15 centres used all available disease modifying therapies. A total number of 7213 people with multiple sclerosis received care in 27 respondent centres. Compared to prevalence estimates, 2500 persons with multiple sclerosis did not receive multiple sclerosis specific care in Hungary.
Conclusion: Less than half of Hungarian care units provided sufficient care for people living with multiple sclerosis. Care units employing fewer neighbouring specialties, might have difficulties diagnosing and providing appropriate care for persons with multiple sclerosis, especially for people with progressive disease course, contributing to the reported low number of persons living with multiple sclerosis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
