

An HDAC9-associated immune-related signature predicts bladder cancer prognosis
- PMID: 35239708
- PMCID: PMC8893690
- DOI: 10.1371/journal.pone.0264527
An HDAC9-associated immune-related signature predicts bladder cancer prognosis
Abstract
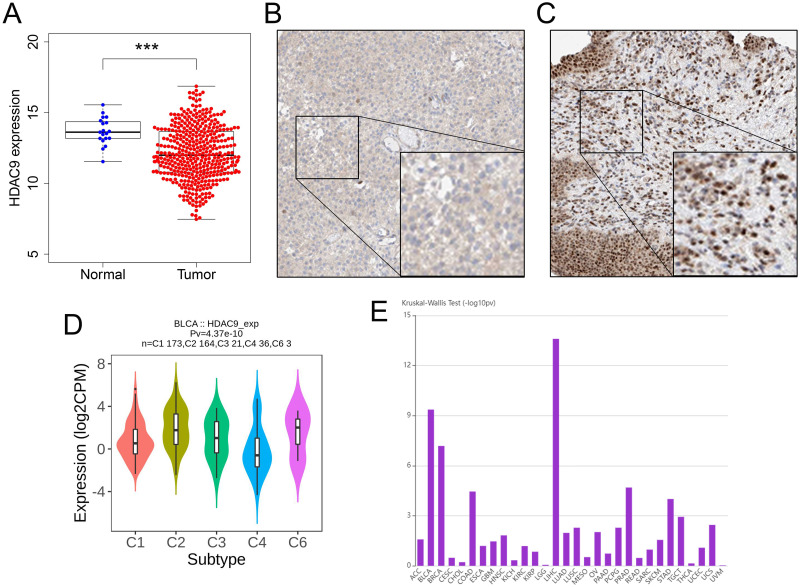
Background: The close relationship between histone deacetylase 9 (HDAC9) and immunity has attracted attention. We constructed an immune signature for HDAC9, a vital epigenetic modification, to predict the survival status and treatment benefits in bladder cancer (BC).
Methods: An exhaustive analysis of HDAC9 and immunology via the tumor and immune system interaction database (TISIDB) was performed, and an immune prognostic risk signature was developed based on genes enriched in the top five immune-related pathways under high HDAC9 status. Comprehensive analysis of survival curves and Cox regression were used to estimate the effectiveness of the risk signature. The relationship between immunological characteristics and the risk score was evaluated, and the mechanisms were also explored.
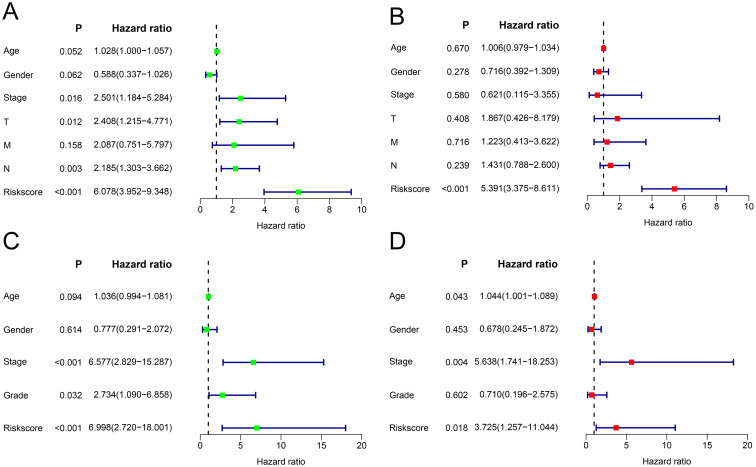
Results: In the TISIDB, HDAC9 was closely related to various immunological characteristics. The risk signature was obtained based on genes related to prognosis enriched in the top five immune-related pathways under high HDAC9 status. The survival rate of the high-risk BC patients was poor. The risk score was closely related to multiple immunological characteristics, drug sensitivity, immunotherapy benefits and biofunctions.
Conclusion: An immune-related prognostic signature established for HDAC9 expression status could independently predict the prognosis of BC patients. The use of this signature could help clinicians make personalized treatment decisions.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures








Similar articles
-
Decreased expression and hypomethylation of HDAC9 lead to poor prognosis and inhibit immune cell infiltration in clear cell renal cell carcinoma.Urol Oncol. 2020 Sep;38(9):740.e1-740.e9. doi: 10.1016/j.urolonc.2020.03.006. Epub 2020 May 8. Urol Oncol. 2020. PMID: 32402768
-
A novel immune-related gene pair prognostic signature for predicting overall survival in bladder cancer.BMC Cancer. 2021 Jul 15;21(1):810. doi: 10.1186/s12885-021-08486-0. BMC Cancer. 2021. PMID: 34266411 Free PMC article.
-
miR-211-5p is down-regulated and a prognostic marker in bladder cancer.J Gene Med. 2020 Dec;22(12):e3270. doi: 10.1002/jgm.3270. Epub 2020 Sep 28. J Gene Med. 2020. PMID: 32893379
-
HDAC9 Inhibition as a Novel Treatment for Stroke.Stroke. 2023 Dec;54(12):3182-3189. doi: 10.1161/STROKEAHA.123.044862. Epub 2023 Nov 9. Stroke. 2023. PMID: 37942644 Review.
-
Histone Deacetylase 9: Its Role in the Pathogenesis of Diabetes and Other Chronic Diseases.Diabetes Metab J. 2020 Apr;44(2):234-244. doi: 10.4093/dmj.2019.0243. Diabetes Metab J. 2020. PMID: 32347025 Free PMC article. Review.
Cited by
-
Identification of a Prognostic Signature Based on Tumor-Infiltrating B Lymphocyte mRNA in Head and Neck Squamous Cell Carcinoma.J Immunol Res. 2025 Mar 19;2025:9375885. doi: 10.1155/jimr/9375885. eCollection 2025. J Immunol Res. 2025. PMID: 40145017 Free PMC article.
-
A lipid metabolism-related risk signature for patients with gliomas constructed with TCGA and CGGA data.Medicine (Baltimore). 2022 Sep 9;101(36):e30501. doi: 10.1097/MD.0000000000030501. Medicine (Baltimore). 2022. PMID: 36086728 Free PMC article.
-
Construction of endothelial cell signatures for predicting the diagnosis, prognosis and immunotherapy response of bladder cancer via machine learning.J Cell Mol Med. 2024 Mar;28(6):e18155. doi: 10.1111/jcmm.18155. J Cell Mol Med. 2024. PMID: 38429911 Free PMC article.
References
-
- von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al.. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol. 2000;18(17):3068–77. Epub 2000/09/23. doi: 10.1200/JCO.2000.18.17.3068 . - DOI - PubMed
-
- Roberts JT, von der Maase H, Sengeløv L, Conte PF, Dogliotti L, Oliver T, et al.. Long-term survival results of a randomized trial comparing gemcitabine/cisplatin and methotrexate/vinblastine/doxorubicin/cisplatin in patients with locally advanced and metastatic bladder cancer. Annals of oncology: official journal of the European Society for Medical Oncology. 2006;17 Suppl 5:v118–22. Epub 2006/06/30. doi: 10.1093/annonc/mdj965 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
