

Differentiation between combined hepatocellular carcinoma and hepatocellular carcinoma: comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017
- PMID: 35241004
- PMCID: PMC8896152
- DOI: 10.1186/s12880-022-00765-x
Differentiation between combined hepatocellular carcinoma and hepatocellular carcinoma: comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017
Erratum in
-
Correction to: Differentiation between combined hepatocellular cholangiocarcinoma and hepatocellular carcinoma: comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017.BMC Med Imaging. 2022 Mar 29;22(1):57. doi: 10.1186/s12880-022-00781-x. BMC Med Imaging. 2022. PMID: 35351025 Free PMC article. No abstract available.
Abstract
Background: The imaging findings of combined hepatocellular cholangiocarcinoma (CHC) may be similar to those of hepatocellular carcinoma (HCC). CEUS LI-RADS may not perform well in distinguishing CHC from HCC. Studies have shown that radiomics has an excellent imaging analysis ability. This study aimed to establish and confirm an ultrasomics model for differentiating CHC from HCC.
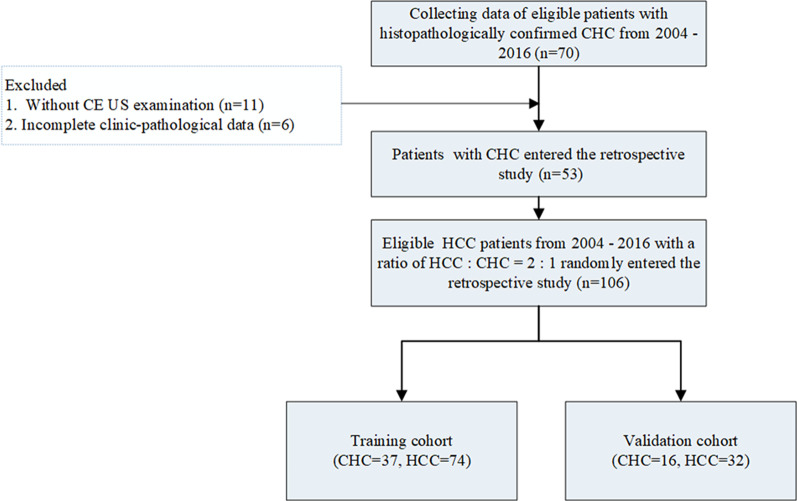
Methods: Between 2004 and 2016, we retrospectively identified 53 eligible CHC patients and randomly included 106 eligible HCC patients with a ratio of HCC:CHC = 2:1, all of whom were categorized according to Contrast-Enhanced (CE) ultrasonography (US) Liver Imaging Reporting and Data System (LI-RADS) version 2017. The model based on ultrasomics features of CE US was developed in 74 HCC and 37 CHC and confirmed in 32 HCC and 16 CHC. The diagnostic performance of the LI-RADS or ultrasomics model was assessed by the area under the curve (AUC), accuracy, sensitivity and specificity.
Results: In the entire and validation cohorts, 67.0% and 81.3% of HCC cases were correctly assigned to LR-5 or LR-TIV contiguous with LR-5, and 73.6% and 87.5% of CHC cases were assigned to LR-M correctly. Up to 33.0% of HCC and 26.4% of CHC were misclassified by CE US LI-RADS. A total of 90.6% of HCC as well as 87.5% of CHC correctly diagnosed by the ultrasomics model in the validation cohort. The AUC, accuracy, sensitivity of the ultrasomics model were higher though without significant difference than those of CE US LI-RADS in the validation cohort.
Conclusion: The proposed ultrasomics model showed higher ability though the difference was not significantly different for differentiating CHC from HCC, which may be helpful in clinical diagnosis.
Keywords: Combined hepatocellular cholangiocarcinoma; Hepatocellular carcinoma; Liver imaging reporting and data system; Ultrasomics.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors do not have any conflicts of interest to declare.
Figures
Similar articles
-
Contrast-enhanced ultrasound in association with serum biomarkers for differentiating combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma and intrahepatic cholangiocarcinoma.World J Gastroenterol. 2020 Dec 14;26(46):7325-7337. doi: 10.3748/wjg.v26.i46.7325. World J Gastroenterol. 2020. PMID: 33362387 Free PMC article.
-
Combined hepatocellular-cholangiocarcinoma: can we use contrast-enhanced ultrasound Liver Imaging Reporting and Data System (LI-RADS) to predict the patient's survival?Eur Radiol. 2021 Aug;31(8):6397-6405. doi: 10.1007/s00330-020-07656-1. Epub 2021 Jan 25. Eur Radiol. 2021. PMID: 33492470
-
Differentiation of hepatocellular carcinoma from intrahepatic cholangiocarcinoma and combined hepatocellular-cholangiocarcinoma in high-risk patients matched to MR field strength: diagnostic performance of LI-RADS version 2018.Abdom Radiol (NY). 2021 Jul;46(7):3168-3178. doi: 10.1007/s00261-021-02996-y. Epub 2021 Mar 3. Abdom Radiol (NY). 2021. PMID: 33660040
-
Diagnostic Performance of CT/MRI Liver Imaging Reporting and Data System v2017 for Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis.Liver Int. 2020 Jun;40(6):1488-1497. doi: 10.1111/liv.14424. Epub 2020 Mar 19. Liver Int. 2020. PMID: 32145134
-
Risk stratification for hepatocellular carcinoma of contrast-enhanced ultrasound Liver Imaging Reporting and Data System (LI-RADS) and the diagnostic performance of LR-5 and LR-M: a systematic review and meta-analysis.Clin Radiol. 2022 Apr;77(4):e280-e286. doi: 10.1016/j.crad.2022.01.041. Epub 2022 Feb 12. Clin Radiol. 2022. PMID: 35164930
Cited by
-
Radiomics Based on Dynamic Contrast-Enhanced Magnetic Resonance Imaging in Preoperative Differentiation of Combined Hepatocellular-Cholangiocarcinoma from Hepatocellular Carcinoma: A Multi-Center Study.J Hepatocell Carcinoma. 2023 Jun 2;10:795-806. doi: 10.2147/JHC.S406648. eCollection 2023. J Hepatocell Carcinoma. 2023. PMID: 37288140 Free PMC article.
-
Correction to: Differentiation between combined hepatocellular cholangiocarcinoma and hepatocellular carcinoma: comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017.BMC Med Imaging. 2022 Mar 29;22(1):57. doi: 10.1186/s12880-022-00781-x. BMC Med Imaging. 2022. PMID: 35351025 Free PMC article. No abstract available.
-
Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma.Diagnostics (Basel). 2023 Apr 20;13(8):1488. doi: 10.3390/diagnostics13081488. Diagnostics (Basel). 2023. PMID: 37189589 Free PMC article. Review.
-
Comparison contrast-enhanced CT with contrast-enhanced US in diagnosing combined hepatocellular-cholangiocarcinoma: a propensity score-matched study.Insights Imaging. 2024 Feb 14;15(1):44. doi: 10.1186/s13244-023-01576-6. Insights Imaging. 2024. PMID: 38353807 Free PMC article.
-
A comparative study between deep learning and radiomics models in grading liver tumors using hepatobiliary phase contrast-enhanced MR images.BMC Med Imaging. 2022 Dec 14;22(1):218. doi: 10.1186/s12880-022-00946-8. BMC Med Imaging. 2022. PMID: 36517762 Free PMC article.
References
-
- He C, Mao Y, Wang J, Song Y, Huang X, Lin X, et al. The predictive value of staging systems and inflammation scores for patients with combined hepatocellular cholangiocarcinoma after surgical resection: a retrospective study. J Gastrointest Surg. 2018;22(7):1239–1250. doi: 10.1007/s11605-018-3756-3. - DOI - PubMed
-
- Zuo HQ, Yan LN, Zeng Y, Yang JY, Luo HZ, Liu JW, et al. Clinicopathological characteristics of 15 patients with combined hepatocellular carcinoma and cholangiocarcinoma. Hepatobiliary Pancreat Dis Int. 2007;6(2):161–165. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
