

Prognostic value and immune relevancy of a combined autophagy-, apoptosis- and necrosis-related gene signature in glioblastoma
- PMID: 35241019
- PMCID: PMC8892733
- DOI: 10.1186/s12885-022-09328-3
Prognostic value and immune relevancy of a combined autophagy-, apoptosis- and necrosis-related gene signature in glioblastoma
Abstract
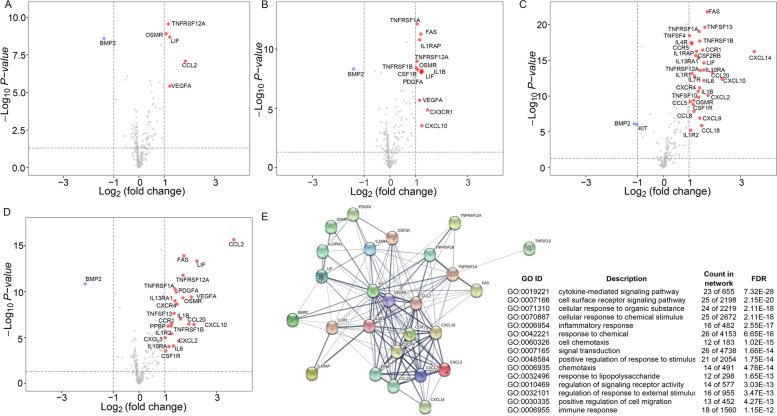
Background: Glioblastoma (GBM) is considered the most malignant and devastating intracranial tumor without effective treatment. Autophagy, apoptosis, and necrosis, three classically known cell death pathways, can provide novel clinical and immunological insights, which may assist in designing personalized therapeutics. In this study, we developed and validated an effective signature based on autophagy-, apoptosis- and necrosis-related genes for prognostic implications in GBM patients.
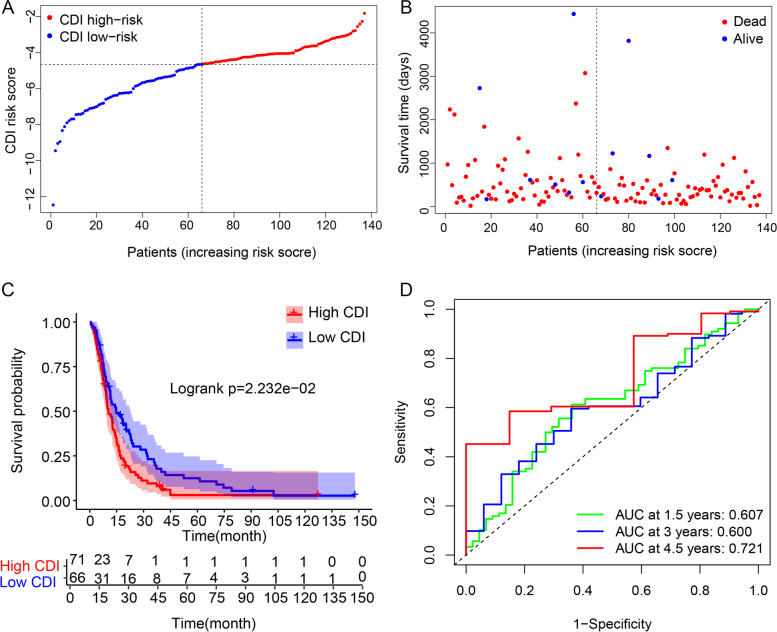
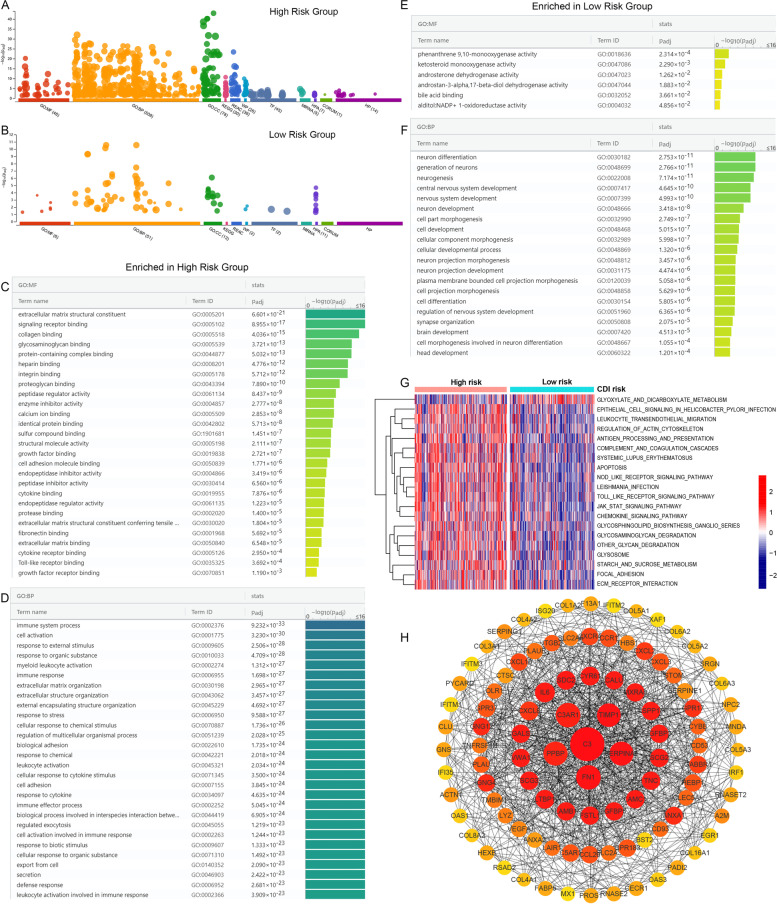
Methods: Variations in the expression of genes involved in autophagy, apoptosis and necrosis were explored in 518 GBM patients from The Cancer Genome Atlas (TCGA) database. Univariate Cox analysis, least absolute shrinkage and selection operator (LASSO) analysis, and multivariate Cox analysis were performed to construct a combined prognostic signature. Kaplan-Meier survival, receiver-operating characteristic (ROC) curves and Cox regression analyses based on overall survival (OS) and progression-free survival (PFS) were conducted to estimate the independent prognostic performance of the gene signature. The Chinese Glioma Genome Atlas (CGGA) dataset was used for external validation. Finally, we investigated the differences in the immune microenvironment between different prognostic groups and predicted potential compounds targeting each group.
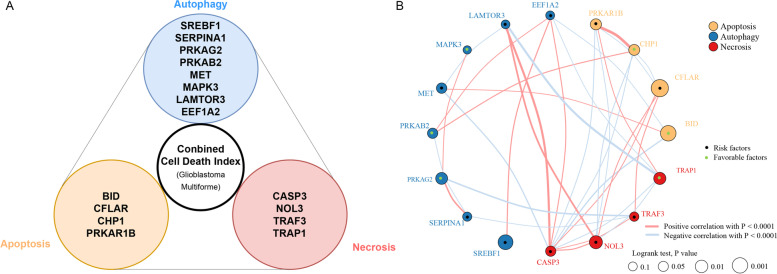
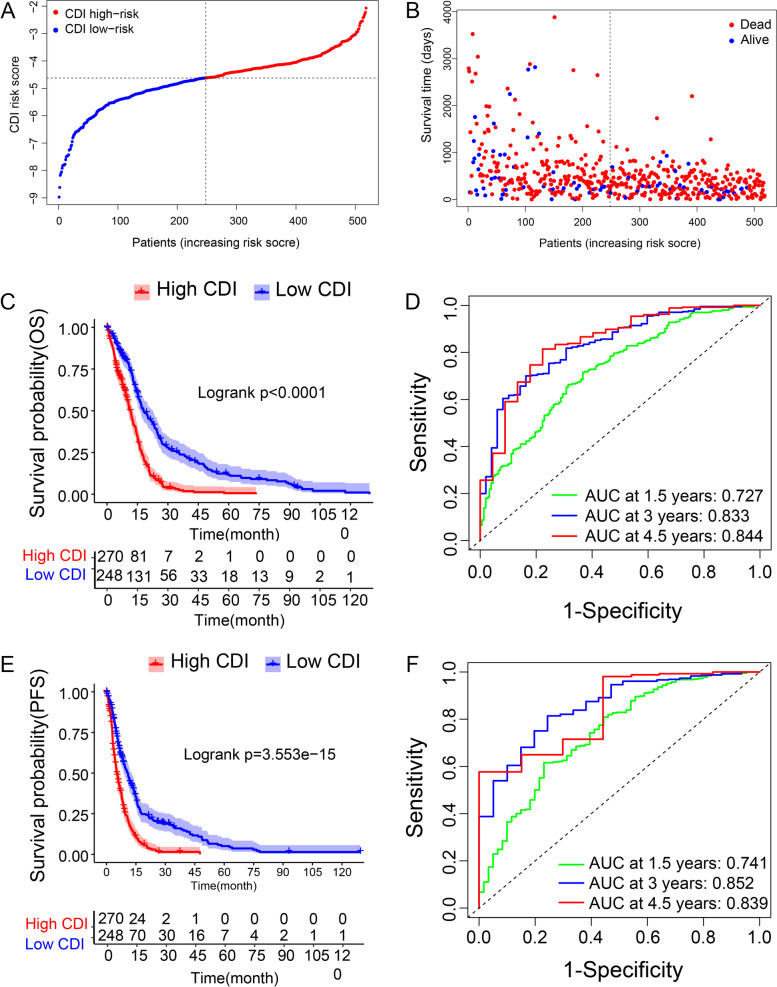
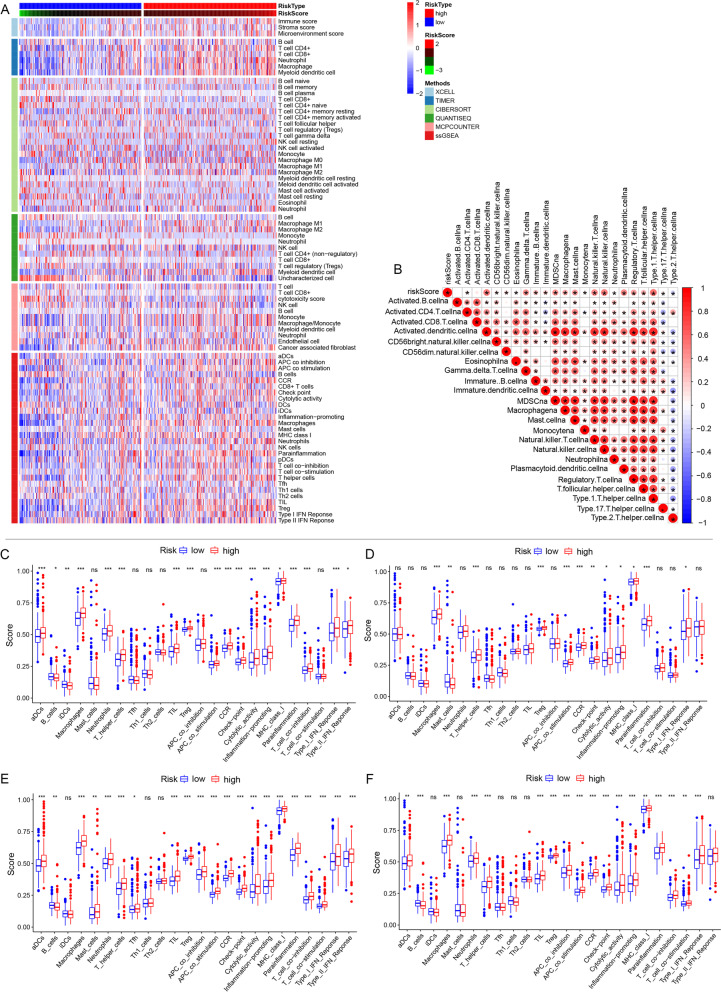
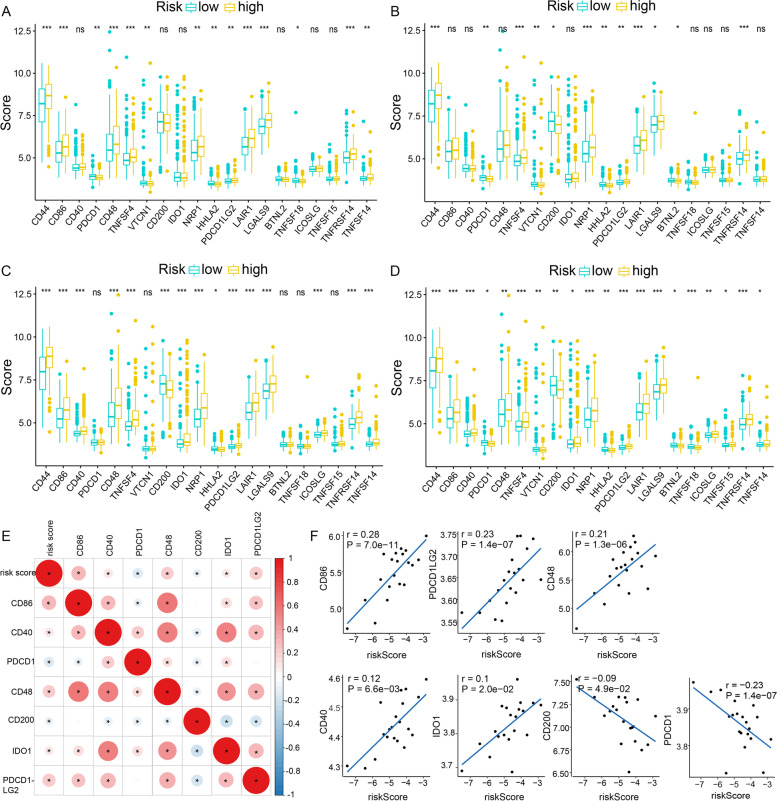
Results: A 16-gene cell death index (CDI) was established. Patients were clustered into either the high risk or the low risk groups according to the CDI score, and those in the low risk group presented significantly longer OS and PFS than the high CDI group. ROC curves demonstrated outstanding performance of the gene signature in both the training and validation groups. Furthermore, immune cell analysis identified higher infiltration of neutrophils, macrophages, Treg, T helper cells, and aDCs, and lower infiltration of B cells in the high CDI group. Interestingly, this group also showed lower expression levels of immune checkpoint molecules PDCD1 and CD200, and higher expression levels of PDCD1LG2, CD86, CD48 and IDO1.
Conclusion: Our study proposes that the CDI signature can be utilized as a prognostic predictor and may guide patients' selection for preferential use of immunotherapy in GBM.
Keywords: CGGA; Cell death index; Glioblastoma (GBM); Immune infiltration; Prognostic; TCGA.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Systematic identification, development, and validation of prognostic biomarkers involving the tumor-immune microenvironment for glioblastoma.J Cell Physiol. 2021 Jan;236(1):507-522. doi: 10.1002/jcp.29878. Epub 2020 Jun 22. J Cell Physiol. 2021. PMID: 32572951
-
Identification of a novel autophagy-related prognostic signature and small molecule drugs for glioblastoma by bioinformatics.BMC Med Genomics. 2022 May 12;15(1):111. doi: 10.1186/s12920-022-01261-5. BMC Med Genomics. 2022. PMID: 35550147 Free PMC article.
-
A novel risk signature with 6 RNA binding proteins for prognosis prediction in patients with glioblastoma.Medicine (Baltimore). 2021 Dec 3;100(48):e28065. doi: 10.1097/MD.0000000000028065. Medicine (Baltimore). 2021. PMID: 35049227 Free PMC article.
-
A Novel Pancreatic Cancer Hypoxia Status Related Gene Signature for Prognosis and Therapeutic Responses.Mol Biotechnol. 2024 Jul;66(7):1684-1703. doi: 10.1007/s12033-023-00807-x. Epub 2023 Jul 5. Mol Biotechnol. 2024. PMID: 37405638 Review.
-
The PTEN-associated immune prognostic signature reveals the landscape of the tumor microenvironment in glioblastoma.J Neuroimmunol. 2023 Mar 15;376:578034. doi: 10.1016/j.jneuroim.2023.578034. Epub 2023 Jan 24. J Neuroimmunol. 2023. PMID: 36791582 Review.
Cited by
-
Gene body hypomethylation of pyroptosis-related genes NLRP7, NLRP2, and NLRP3 facilitate non-invasive surveillance of hepatocellular carcinoma.Funct Integr Genomics. 2023 Jun 5;23(2):198. doi: 10.1007/s10142-023-01114-z. Funct Integr Genomics. 2023. PMID: 37273114
-
A lipid metabolism-related risk signature for patients with gliomas constructed with TCGA and CGGA data.Medicine (Baltimore). 2022 Sep 9;101(36):e30501. doi: 10.1097/MD.0000000000030501. Medicine (Baltimore). 2022. PMID: 36086728 Free PMC article.
-
Integrated analysis reveals the potential of cluster of differentiation 86 as a key biomarker in high-grade glioma.Aging (Albany NY). 2023 Dec 26;15(24):15402-15418. doi: 10.18632/aging.205359. Epub 2023 Dec 26. Aging (Albany NY). 2023. PMID: 38154107 Free PMC article.
-
Analysis of cell death-related genes to evaluate the prognostic and immunotherapeutic value in bladder cancer.Heliyon. 2024 Jun 17;10(12):e33200. doi: 10.1016/j.heliyon.2024.e33200. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 39005901 Free PMC article.
-
Hirudin inhibits glioma growth through mTOR-regulated autophagy.J Cell Mol Med. 2023 Sep;27(18):2701-2713. doi: 10.1111/jcmm.17851. Epub 2023 Aug 4. J Cell Mol Med. 2023. PMID: 37539490 Free PMC article.
References
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359(5):492–507. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
