

Distress financing in coping with out-of-pocket expenditure for maternity care in India
- PMID: 35241077
- PMCID: PMC8892690
- DOI: 10.1186/s12913-022-07656-5
Distress financing in coping with out-of-pocket expenditure for maternity care in India
Abstract
Background: The cost of maternity care is seen as the barrier in utilizing maternity care, resulting in high maternal deaths. This study focuses on the distress financing and its coping mechanisms associated with maternity care expenditure in India so that corrective measures can be taken to reduce the burden of maternity care.
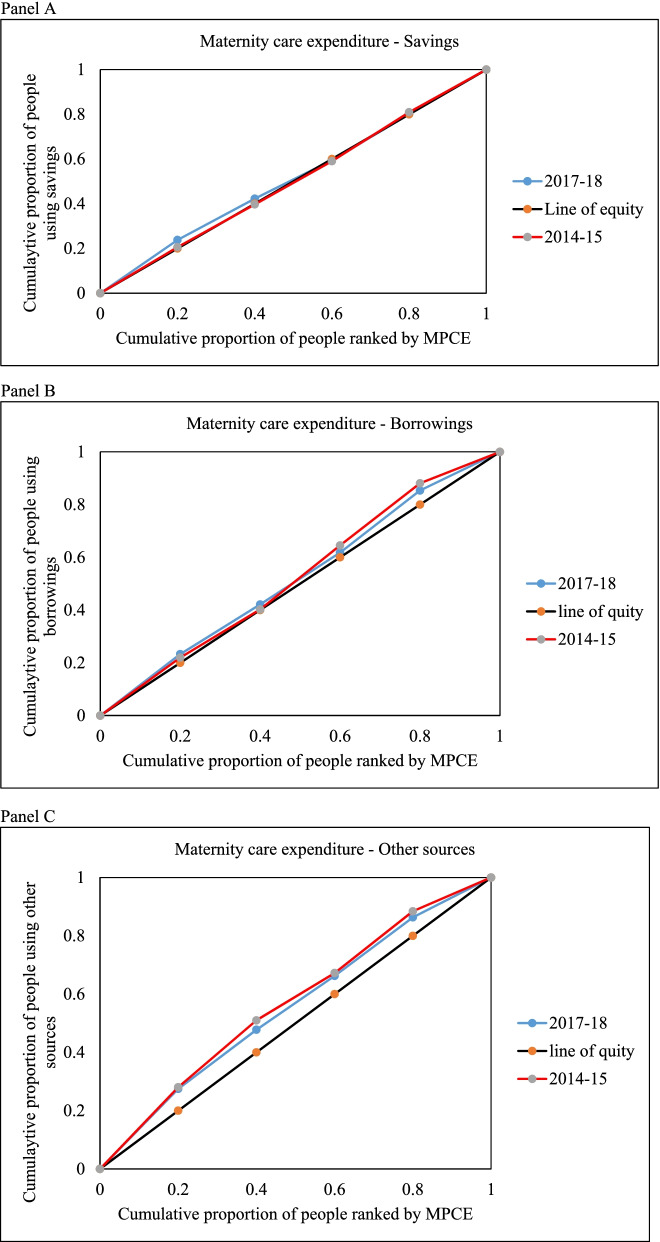
Methods: This study used the National Sample Survey (NSS) data conducted in 20,014-15 (71st round of NSS) and 2017-18(75th round of NSS). We define distress financing as use of formal borrowing, borrowing from friends or family or sale of asser to finance maternity care. Percentage of pregnant/delivered females using distress financing were calculated.. The present study also used multinomial logistic regression with 95% to understand the impact of socio-economic variables on distress financing and concentration index to measure the inequality in maternity care expenditure.
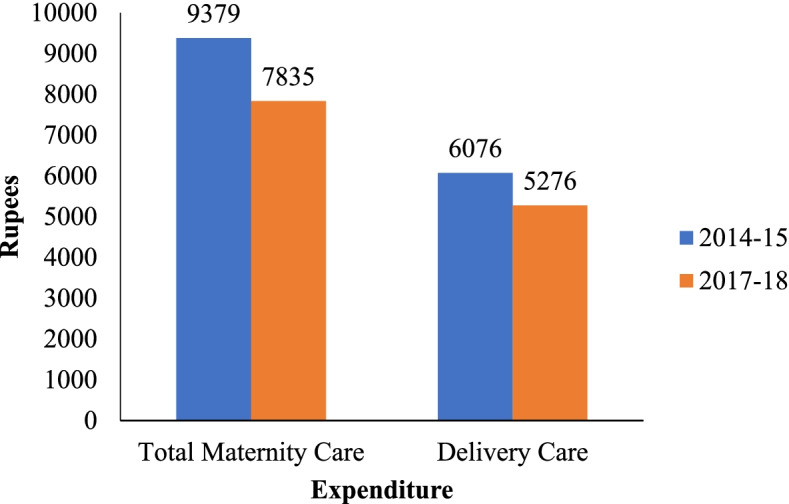
Results: This study found that the maternity care expenditure has decreased from the INR. 9379 in 2014-15 to INR. 7835 in 2017-18. The percentage of households using distress financing is higher among the poorest (13.2%). Almost 14% of the SC households experience distress financing. Among EAG + A states, particularly in Madhya Pradesh and Uttarakhand, the percentage of households are which experience a high level of distress financing increased from 8.9 to 18.3 and 0.7 to 8.1 from 2014-15 to 2017-18 respectively. The study finds that more urban households (37%) utilized insurance than rural households (26%). Among EAG + A states, 67.9 percent of households were dependent upon household savings, and it was 63.6 percent in the non-EAG states. The households with a high burden of maternity care expenditure were at higher risk of borrowing money to finance the cost of maternity as compared to use of savings/income for the same (relative risk (RR) (R: 2.59; P < 0.01; 95% CI: 2.15-3.13). Mothers belonging to the SC caste were at significantly higher risk (RR: 1.43; P < 0.1; 95% CI: 1.07-1.91). of using borrowings as compared to the use of income/savings. Mothers with college education were 50% more likely to use health insurance as compared to those with primary education.
Conclusions: The study found that even though many programs for maternity care services are there, the maternity care expenditure, particularly the delivery care expenses, is very high in many states. The study recommends that India should increase subsidized maternity care facilities to decrease catastrophic maternity expenditure among households.
Keywords: Coping Mechanism; Distress Financing; Expenditure; Maternity care.
© 2022. The Author(s).
Conflict of interest statement
We declare that We have no competing interests.
Figures


References
-
- World Health Organization . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. 2019.
-
- Special bulletin on maternal mortality in India 2016–18 https://censusindia.gov.in/vital_statistics/SRS_Bulletins/MMR%20Bulletin... . Accessed on 25 August 2021
-
- Schwartz DA. Hypertensive Mothers, Obstetric Hemorrhage, and Infections: Biomedical Aspects of Maternal Death Among Indigenous Women in Mexico and Central America. In Maternal Death and Pregnancy-Related Morbidity Among Indigenous Women of Mexico and Central America. Cham: Springer; 2018. pp. 35–50.
MeSH terms
LinkOut - more resources
Full Text Sources
