

Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis
- PMID: 35241426
- PMCID: PMC9120409
- DOI: 10.1136/annrheumdis-2021-221664
Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis
Abstract
Objective: To evaluate the efficacy and safety of an oral selective tyrosine kinase 2 (TYK2) inhibitor, deucravacitinib, in patients with active psoriatic arthritis (PsA).
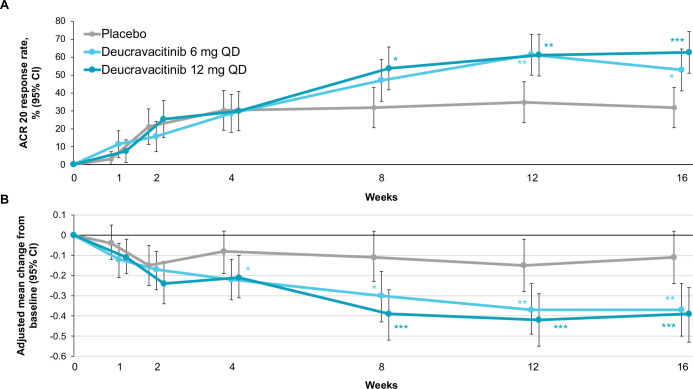
Methods: In this double-blind, phase II trial, 203 patients with PsA were randomised 1:1:1 to placebo, deucravacitinib 6 mg once a day or 12 mg once a day. The primary endpoint was American College of Rheumatology-20 (ACR-20) response at week 16.
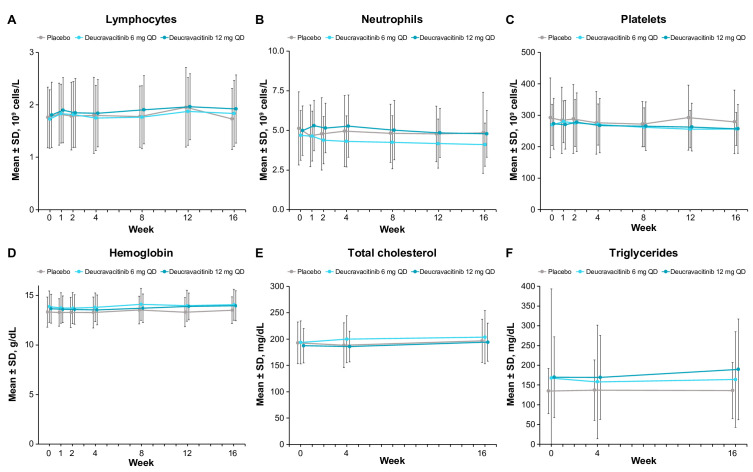
Results: ACR-20 response was significantly higher with deucravacitinib 6 mg once a day (52.9%, p=0.0134) and 12 mg once a day (62.7%, p=0.0004) versus placebo (31.8%) at week 16. Both deucravacitinib doses resulted in significant improvements versus placebo (p≤0.05) in the multiplicity-controlled secondary endpoints of change from baseline in Health Assessment Questionnaire-Disability Index and Short Form-36 Physical Component Summary score and in Psoriasis Area and Severity Index-75 response. Improvements were also seen in multiple exploratory endpoints with deucravacitinib treatment. The most common adverse events (AEs) (≥5%) in deucravacitinib-treated patients were nasopharyngitis, upper respiratory tract infection, sinusitis, bronchitis, rash, headache and diarrhoea. There were no serious AEs and no occurrence of herpes zoster, opportunistic infections and major adverse cardiovascular events, or differences versus placebo in mean changes in laboratory parameters with deucravacitinib treatment.
Conclusions: Treatment with the selective TYK2 inhibitor deucravacitinib was well tolerated and resulted in greater improvements than placebo in ACR-20, multiplicity-controlled secondary endpoints and other exploratory efficacy measures in patients with PsA. Larger trials over longer periods of time with deucravacitinib are warranted to confirm its safety profile and benefits in PsA.
Trial registration number: NCT03881059.
Keywords: arthritis; inflammation; psoriatic; therapeutics.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: PJM: research grants: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, SUN Pharma and UCB; consulting and/or speaker fees: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, SUN Pharma and UCB. AAD: consulting and/or advisory boards: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, GlaxoSmithKline, Janssen, Novartis, Pfizer and UCB; research grants: AbbVie, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer and UCB. DvdH: consulting fees: AbbVie, Amgen, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Boehringer Ingelheim, Celgene, Cyxone, Daiichi, Eisai, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi, Takeda and UCB Pharma; Director: Imaging Rheumatology. FB: research grants: Pfizer, Janssen, Chugai, Celgene and Roche; consultancies/speaker fees: Pfizer, AbbVie, Sanofi, Lilly, Novartis, Genzyme, Boehringer, Janssen, MSD, Celgene, Roche, Chugai, Bristol Myers Squibb and UCB Pharma. AJK: shareholder: Pfizer, Sanofi, GlaxoSmithKline, Gilead Sciences and Novartis; paid consultant: AbbVie, Boehringer Ingelheim, Flexion, Janssen, Pfizer, Sanofi, Regeneron, SUN Pharma Advanced Research and Gilead Sciences; speakers bureau: Celgene, Merck, Lilly, Novartis, Pfizer, Sanofi, Genzyme, Flexion and AbbVie. JN: research grants to foundation: AbbVie, Amgen, Eli Lilly, Genentech, Novartis, UCB, Pfizer, Gilead and Bristol Myers Squibb. SS, MN, SB: employees and shareholders of Bristol Myers Squibb. JK: employee of Bristol Myers Squibb at time of the study conduct.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
