

Spontaneous tumor regression following COVID-19 vaccination
- PMID: 35241495
- PMCID: PMC8896046
- DOI: 10.1136/jitc-2021-004371
Spontaneous tumor regression following COVID-19 vaccination
Abstract
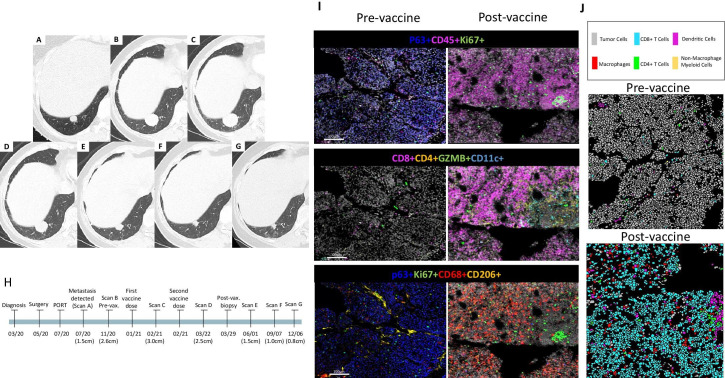
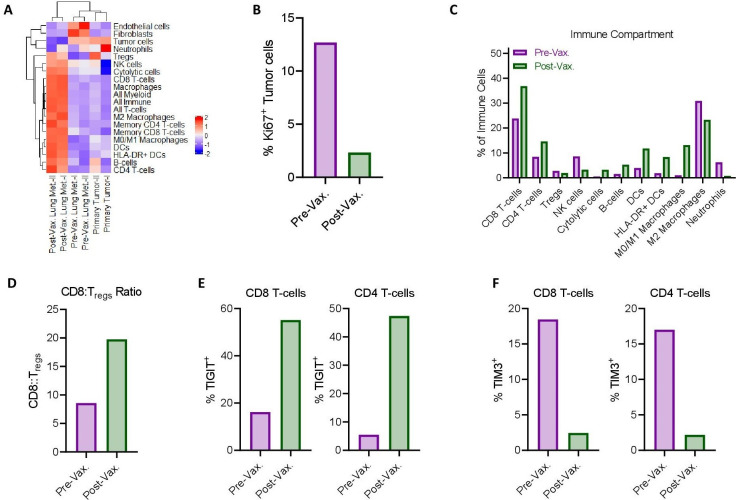
Vaccination against COVID-19 is critical for immuno-compromised individuals, including patients with cancer. Systemic reactogenicity, a manifestation of the innate immune response to vaccines, occurs in up to 69% of patients following vaccination with RNA-based COVID-19 vaccines. Tumor regression can occur following an intense immune-inflammatory response and novel strategies to treat cancer rely on manipulating the host immune system. Here, we report spontaneous regression of metastatic salivary gland myoepithelial carcinoma in a patient who experienced grade 3 systemic reactogenicity, following vaccination with the mRNA-1273 COVID-19 vaccine. Histological and immunophenotypic inspection of the postvaccination lung biopsy specimens showed a massive inflammatory infiltrate with scant embedded tumor clusters (<5%). Highly multiplexed imaging mass cytometry showed that the postvaccination lung metastasis samples had remarkable immune cell infiltration, including CD4+ T cells, CD8+ T cells, natural killer cells, B cells, and dendritic cells, which contrasted with very low levels of these cells in the prevaccination primary tumor and lung metastasis samples. CT scans obtained 3, 6, and 9 months after the second vaccine dose demonstrated persistent tumor shrinkage (50%, 67%, and 73% reduction, respectively), suggesting that vaccination stimulated anticancer immunity. Insight: This case suggests that the mRNA-1273 COVID-19 vaccine stimulated anticancer immunity and tumor regression.
Keywords: COVID-19; head and neck neoplasms; immunogenicity; translational medical research; tumor microenvironment; vaccine.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RF: reports personal fees from Regeneron-Sanofi, Ayala Pharmaceuticals, Prelude Pharmaceuticals, Bicara Therapeutics, Klus Pharma, Medscape, Carevive, Merck, and Guidepoint Global and institutional fees from AstraZeneca, Merck, Genentech, Pfizer, EMD-Serono, Ayala Pharmaceuticals, Prelude Pharmaceuticals, and Rakuten Medical not related to the topic of the submitted work.
Figures
References
-
- Coley WB. The treatment of malignant tumors by repeated inoculations of erysipelas: with a report of ten original cases. Am J Med Sci 1893;105:487. - PubMed
-
- Guidance for industry: toxicity grading scale for healthy adult and adolescent volunteers enrolled in preventive vaccine clinical trials 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials