

A unique case of thoracic endometriosis syndrome and pulmonary Langerhans' cell histiocytosis: Six recurrent pneumothoraces
- PMID: 35242517
- PMCID: PMC8866092
- DOI: 10.1016/j.rmcr.2022.101603
A unique case of thoracic endometriosis syndrome and pulmonary Langerhans' cell histiocytosis: Six recurrent pneumothoraces
Abstract
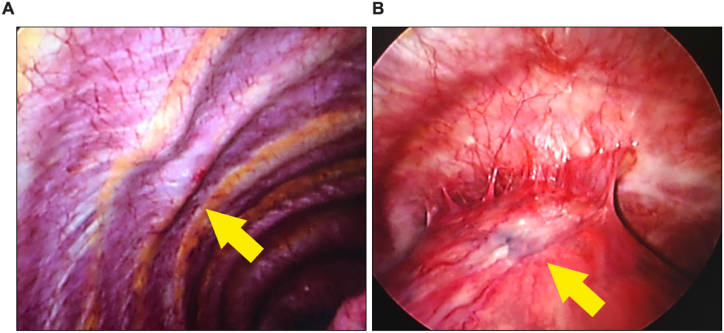
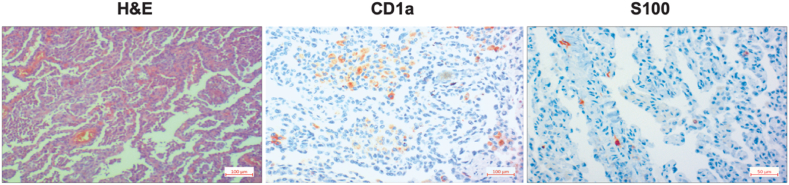
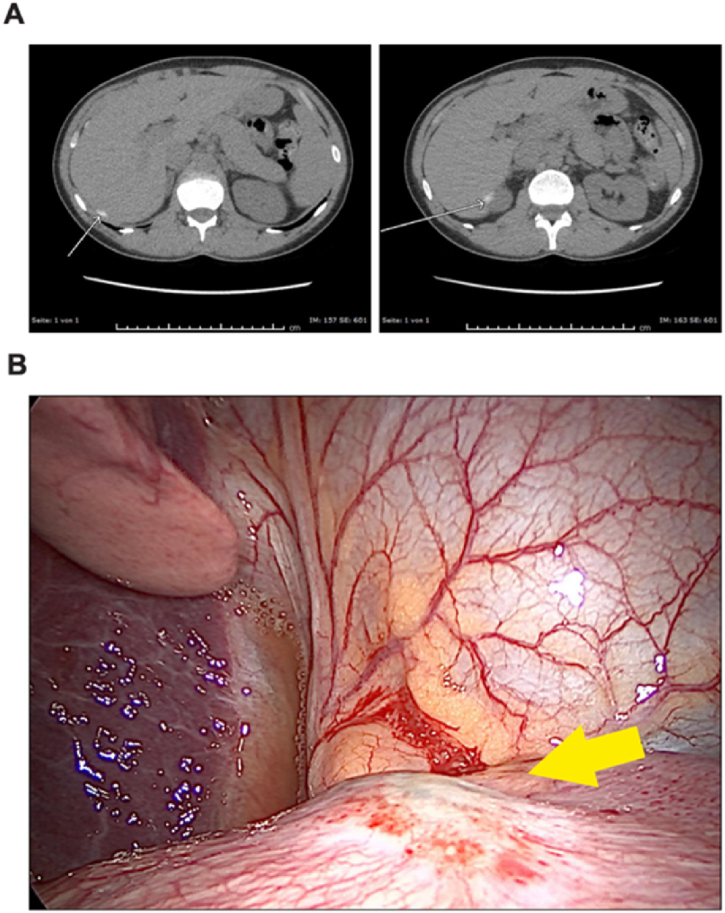
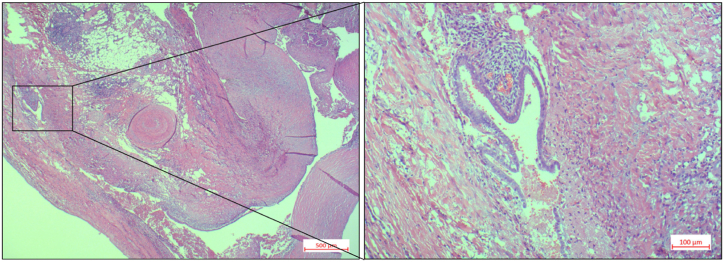
Spontaneous pneumothorax (SP) in women of reproductive age with causes such as thoracic endometriosis syndrome (TES) presents a diagnostic and therapeutic challenge. A 33-year-old women was treated conservatively with chest tube insertion for a first occurrence of a right-sided pneumothorax in September 2015. In January 2016, a right-sided video-assisted thoracoscopic surgery (VATS) wedge resection and partial parietal pleurectomy was performed due to a recurrence. A right-sided VATS was again performed in December 2016 with multiple wedge resections and a total pleurectomy revealing a pulmonary Langerhans' cell histiocytosis (PLCH) in the histological and immunohistochemical examinations. The patient was recommended an abstinence of smoking and further course was unremarkable until May 2019, when due to a recurrent pneumothorax, she received a talc pleurodesis via right-sided VATS. Due to yet another recurrence, she underwent a talc slurry pleurodesis over a right sided chest drain. In March 2020 due to recurrence, a right-sided VATS was performed and a blueish nodular lesion was resected from the diaphragm. The histological examination revealed an endometriosis with a diagnosis of TES. Since the patient did not exhibit a temporal relationship between her periods and the onset of pneumothorax symptoms, a final diagnosis of non-catamenial endometriosis-related pneumothorax was made. The patient is currently continuing smoking abstinence and is under hormone therapy. She has not presented with a recurrence. In clinical practice, it is important not to just relay on the information available to us, but to reevaluate the patient history to uncover new clues leading to a new diagnosis.
Keywords: Pulmonary Langerhans' cell histiocytosis (PLCH); Spontaneous pneumothorax (SP); Thoracic endometriosis syndrome (TES); Video-assisted thoracoscopic surgery (VATS).
© 2022 Published by Elsevier Ltd.
Figures
References
-
- Shrestha B., Shrestha S., Peters P., Ura M., Windsor M., Naidoo R. Catamenial pneumothorax, a commonly misdiagnosed thoracic condition: multicentre experience and audit of a small case series with review of the literature. Heart Lung Circ. 2019;28(6):850–857. doi: 10.1016/j.hlc.2019.01.012. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
