

Arrhythmias in Patients With Valvular Heart Disease: Gaps in Knowledge and the Way Forward
- PMID: 35242822
- PMCID: PMC8885812
- DOI: 10.3389/fcvm.2022.792559
Arrhythmias in Patients With Valvular Heart Disease: Gaps in Knowledge and the Way Forward
Abstract
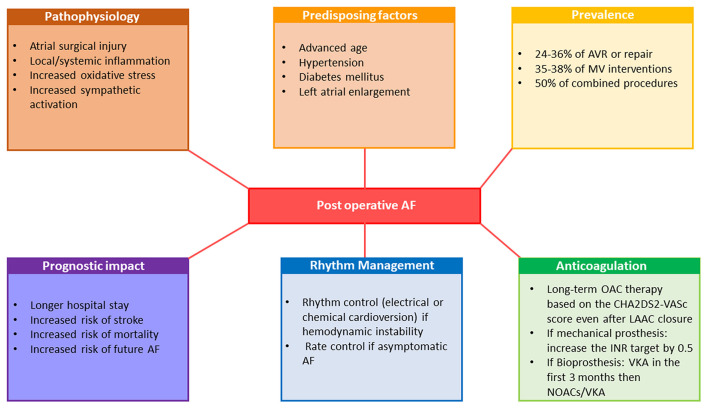
The prevalence of both organic valvular heart disease (VHD) and cardiac arrhythmias is high in the general population, and their coexistence is common. Both VHD and arrhythmias in the elderly lead to an elevated risk of hospitalization and use of health services. However, the relationships of the two conditions is not fully understood and our understanding of their coexistence in terms of contemporary management and prognosis is still limited. VHD-induced left ventricular dysfunction/hypertrophy and left atrial dilation lead to both atrial and ventricular arrhythmias. On the other hand, arrhythmias can be considered as an independent condition resulting from a coexisting ischemic or non-ischemic substrate or idiopathic ectopy. Both atrial and ventricular VHD-induced arrhythmias may contribute to clinical worsening and be a turning point in the natural history of VHD. Symptoms developed in patients with VHD are not specific and may be attributable to hemodynamical consequences of valve disease but also to other cardiac conditions including arrhythmias which are notably prevalent in this population. The issue how to distinguish symptoms related to VHD from those related to atrial fibrillation (AF) during decision making process remains challenging. Moreover, AF is a traditional limit of echocardiography and an important source of errors in assessment of the severity of VHD. Despite recent progress in understanding the pathophysiology and prognosis of postoperative AF, many questions remain regarding its prevention and management. Furthermore, life-threatening ventricular arrhythmias can predispose patients with VHD to sudden cardiac death. Evidence for a putative link between arrhythmias and outcome in VHD is growing but available data on targeted therapies for VHD-related arrhythmias, including monitoring and catheter ablation, is scarce. Despite growing evidences, more research focused on the prognosis and optimal management of VHD-related arrhythmias is still required. We aimed to review the current evidence and identify gaps in knowledge about the prevalence, prognostic considerations, and treatment of atrial and ventricular arrhythmias in common subtypes of organic VHD.
Keywords: aortic stenosis; arrhythmic mitral valve prolapse; atrial arrhythmia; postoperative atrial fibrillation; valvular heart disease; ventricular arrhythmia.
Copyright © 2022 Kubala, de Chillou, Bohbot, Lancellotti, Enriquez-Sarano and Tribouilloy.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Banerjee A, Allan V, Denaxas S, Shah A, Kotecha D, Lambiase PD, et al. Subtypes of atrial fibrillation with concomitant valvular heart disease derived from electronic health records: phenotypes, population prevalence, trends and prognosis. Europace. (2019) 21:1776–84. 10.1093/europace/euz220 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources