

BRCA1/2 Mutations and Cardiovascular Function in Breast Cancer Survivors
- PMID: 35242827
- PMCID: PMC8885808
- DOI: 10.3389/fcvm.2022.833171
BRCA1/2 Mutations and Cardiovascular Function in Breast Cancer Survivors
Abstract
Objective: Animal models suggest that BRCA1/2 mutations increase doxorubicin-induced cardiotoxicity risk but data in humans are limited. We aimed to determine whether germline BRCA1/2 mutations are associated with cardiac dysfunction in breast cancer survivors.
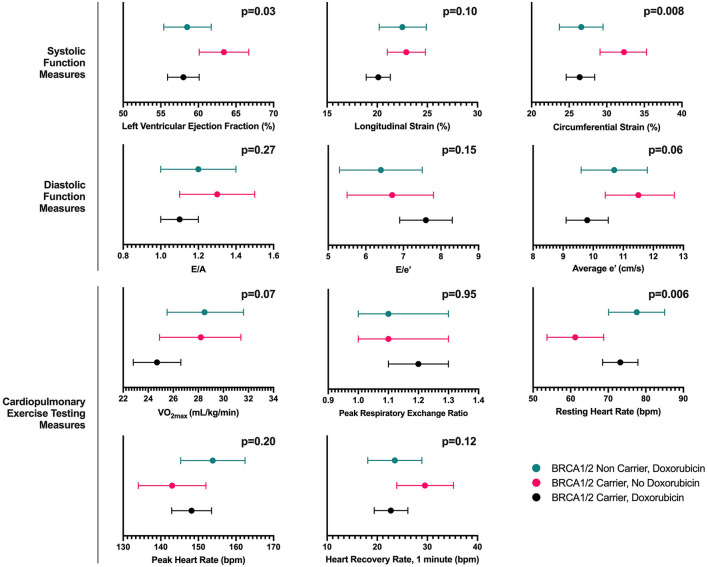
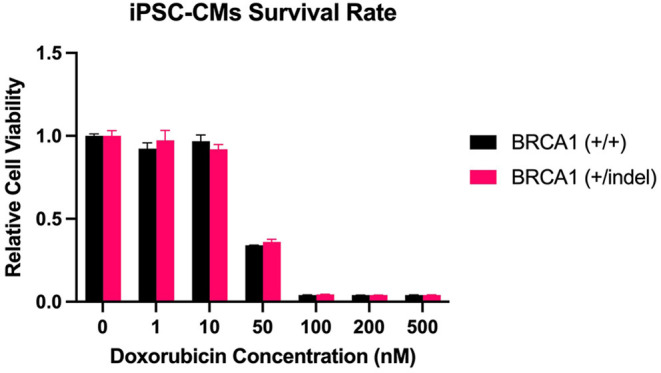
Methods: In a single-center cross-sectional study, stage I-III breast cancer survivors were enrolled according to three groups: (1) BRCA1/2 mutation carriers treated with doxorubicin; (2) BRCA1/2 mutation non-carriers treated with doxorubicin; and (3) BRCA1/2 mutation carriers treated with non-doxorubicin cancer therapy. In age-adjusted analysis, core-lab quantitated measures of echocardiography-derived cardiac function and cardiopulmonary exercise testing (CPET) were compared across the groups. A complementary in vitro study was performed to assess the impact of BRCA1 loss of function on human induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs) survival following doxorubicin exposure.
Results: Sixty-seven women with mean (standard deviation) age of 50 (11) years were included. Age-adjusted left ventricular ejection fraction (LVEF) was lower in participants receiving doxorubicin regardless of BRCA1/2 mutation status (p = 0.03). In doxorubicin-treated BRCA1/2 mutation carriers and non-carriers, LVEF was lower by 5.4% (95% CI; -9.3, -1.5) and 4.8% (95% CI; -9.1, -0.5), respectively compared to carriers without doxorubicin exposure. No significant differences in VO2max were observed across the three groups (poverall = 0.07). Doxorubicin caused a dose-dependent reduction in viability of iPSC-CMs in vitro without differences between BRCA1 mutant and wild type controls (p > 0.05).
Conclusions: BRCA1/2 mutation status was not associated with differences in measures of cardiovascular function or fitness. Our findings do not support a role for increased cardiotoxicity risk with BRCA1/2 mutations in women with breast cancer.
Keywords: BRCA1/2; HER2 therapy; anthracycline; breast cancer; cardiomyocyte; heart failure.
Copyright © 2022 Demissei, Lv, Wilcox, Sheline, Smith, Sturgeon, McDermott-Roe, Musunuru, Lefebvre, Domchek, Shah and Ky.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous