

Evaluation of image-guided and surface-guided radiotherapy for breast cancer patients treated in deep inspiration breath-hold: A single institution experience
- PMID: 35243045
- PMCID: PMC8861395
- DOI: 10.1016/j.tipsro.2022.02.001
Evaluation of image-guided and surface-guided radiotherapy for breast cancer patients treated in deep inspiration breath-hold: A single institution experience
Erratum in
-
Corrigendum to "Evaluation of image-guided and surface-guided radiotherapy for breast cancer patients treated in deep inspiration breath-hold: A single institution experience" [Tech. Innov. Patient Support Radiat. Oncol. 21 (2022) 51-57].Tech Innov Patient Support Radiat Oncol. 2023 Jan 7;25:100198. doi: 10.1016/j.tipsro.2022.12.005. eCollection 2023 Mar. Tech Innov Patient Support Radiat Oncol. 2023. PMID: 36654719 Free PMC article.
Abstract
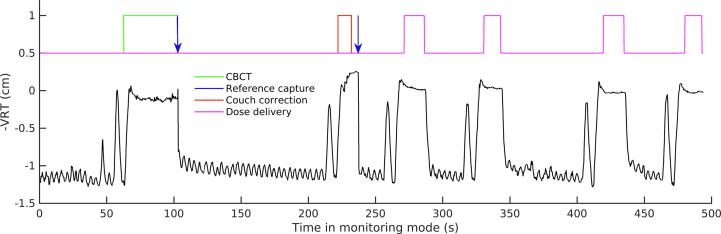
Introduction: Nowadays, deep inspiratory breath-hold is a common technique to reduce heart dose in left-sided breast radiotherapy. This study evaluates the evolution of the breath-hold technique in our institute, from portal imaging during dose delivery to continuous monitoring with surface-guided radiotherapy (SGRT).
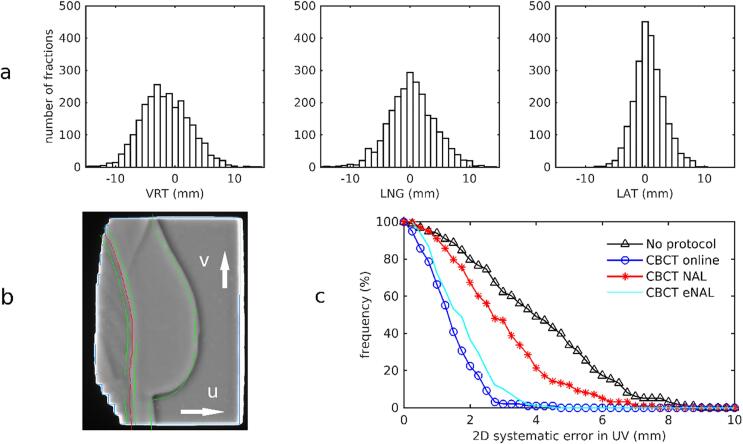
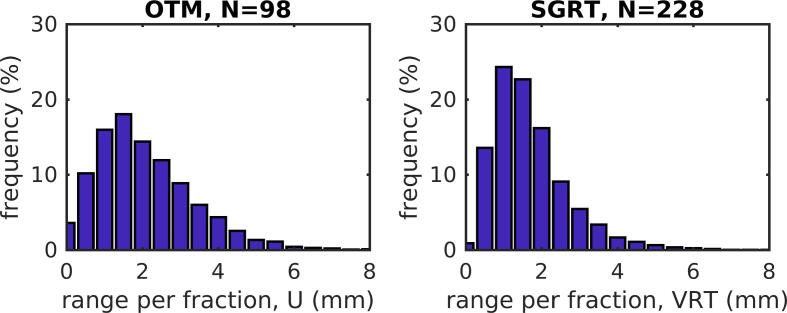
Materials and methods: Setup data and portal imaging results were analyzed for 98 patients treated before 2014, and SGRT data for 228 patients treated between 2018 and 2020. For the pre-SGRT group, systematic and random setup errors were calculated for different correction protocols. Residual errors and reproducibility of breath-holds were evaluated for both groups. The benefit of using SGRT for initial positioning was evaluated for another cohort of 47 patients.
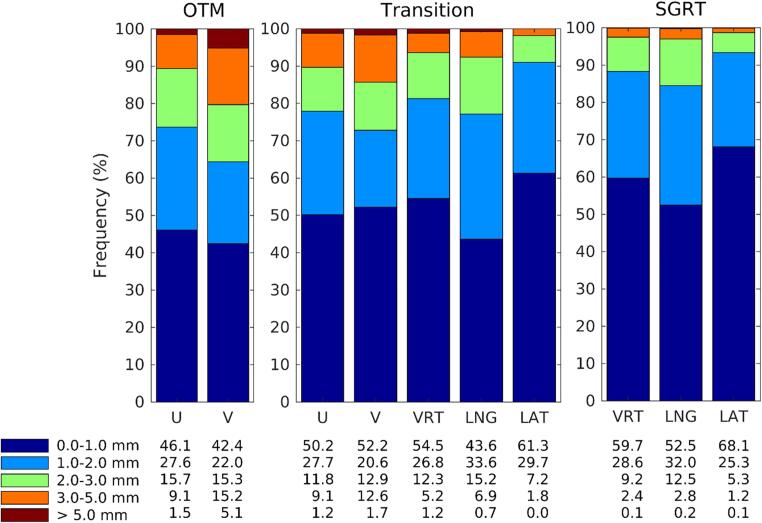
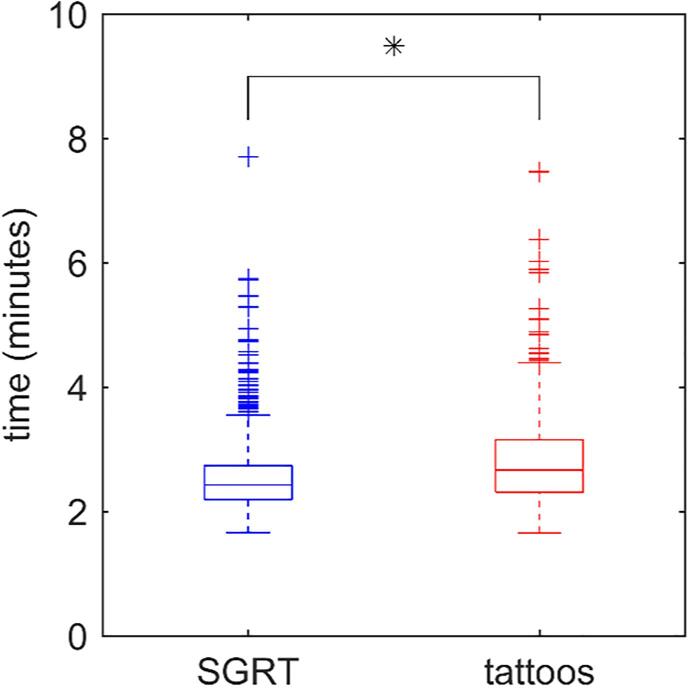
Results: Online correction reduced the population mean error from 3.9 mm (no corrections) to 1.4 mm. Despite online setup correction, deviations greater than 3 mm were observed in about 10% and 20% of the treatment beams in ventral-dorsal and cranial-caudal directions, respectively. However, these percentages were much smaller than with offline protocols or no corrections. Mean absolute differences between breath-holds within a fraction were smaller in the SGRT-group (1.69 mm) than in the pre-SGRT-group (2.10 mm), and further improved with addition of visual feedback (1.30 mm). SGRT for positioning did not improve setup accuracy, but slightly reduced the time for imaging and setup correction, allowing completion within 3.5 min for 95% of fractions.
Conclusion: For accurate radiotherapy breast treatments using deep inspiration breath-hold, daily imaging and correction is required. SGRT provides accurate information on patient positioning during treatment and improves patient compliance with visual feedback.
Keywords: (U, V), ventral-dorsal and cranial-caudal direction in the tangential beam, respectively; Breast; Breath-hold; CBCT, cone-beam CT; CT, computer tomography; DIBH; DIBH, Deep inspiratory breath-hold; DRRs, digitally reconstructed radiographs; LAT, medio-lateral direction; LNG, cranial-caudal direction; NAL, no-action-level setup correction protocol; OTM, online treatment monitor; SGRT, surface-guided radiotherapy; Surface-guided radiotherapy; VRT, anterior-posterior direction; eNAL, extended NAL setup correction protocol.
© 2022 The Authors. Published by Elsevier B.V. on behalf of European Society for Radiotherapy & Oncology.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: The department has research collaborations with Elekta AB, Accuray Inc, VisionRT, and Varian Medical Systems.
Figures
References
-
- Darby S., McGale P., Correa C., Taylor C., Arriagada R., Clarke M., et al. Effect of radiotherapy after breast-conserving surgery on 10 year recurrence and 15 year breast cancer death: meta-analysis of individual patient data for 10 801 women in 17 randomised trials. Lancet. 2011;378:1707–1716. doi: 10.1016/S0140-6736(11)61629-2. - DOI - PMC - PubMed
-
- Lu H.-M., Cash E., Chen M.H., Chin L., Manning W.J., Harris J., et al. Reduction of cardiac volume in left-breast treatment fields by respiratory maneuvers: a CT study. Int J Radiat Oncol Biol Phys. 2000;47(4):895–904. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
