

Chronic invasive fungal sinusitis with orbital and olfactory cleft involvement secondary to indolent mucormycosis
- PMID: 35243178
- PMCID: PMC8881357
- DOI: 10.1016/j.ajoc.2022.101448
Chronic invasive fungal sinusitis with orbital and olfactory cleft involvement secondary to indolent mucormycosis
Abstract
Purpose: Chronic invasive fungal sinusitis secondary to indolent mucormycosis is a rare clinical entity, and the ideal management is controversial. A case of indolent mucormycosis successfully managed with conservative debridement and retrobulbar amphotericin B is herein reported.
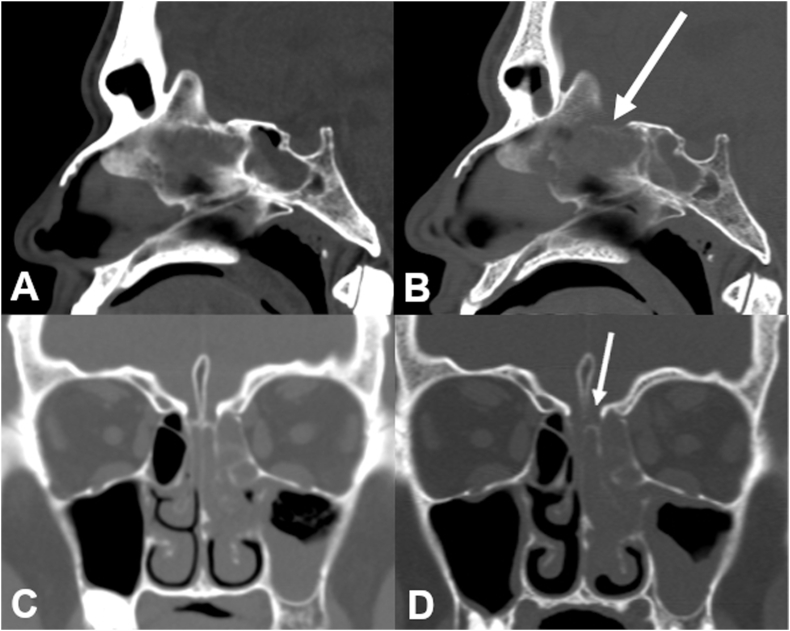
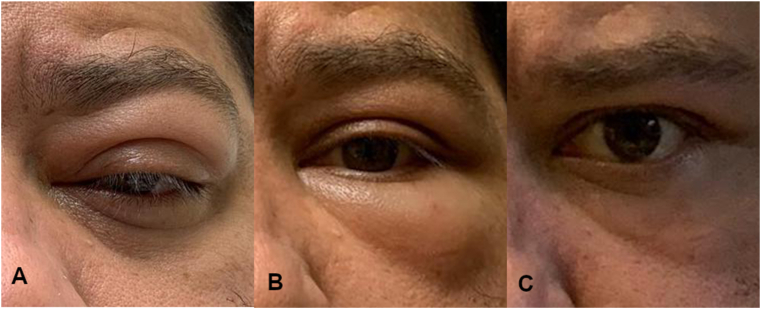
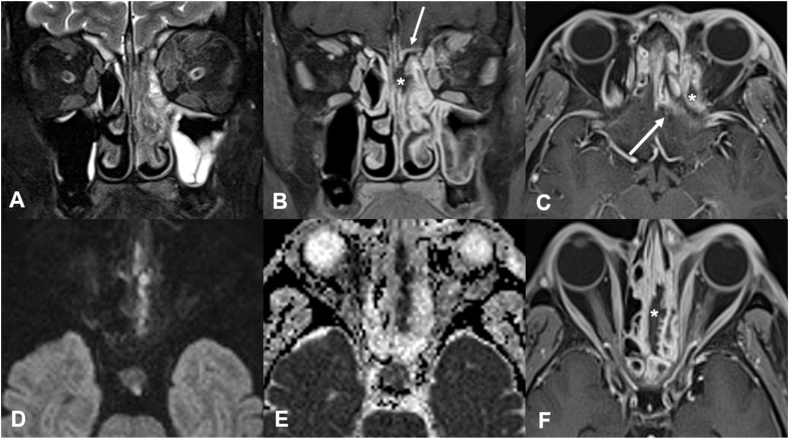
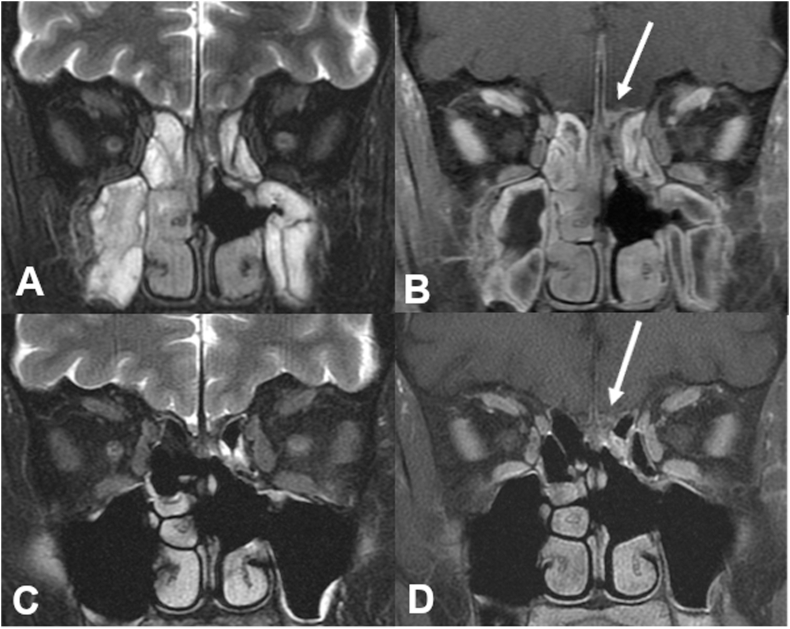
Observations: A 42-year-old man with diabetes mellitus and kidney transplant presented with chronic invasive fungal sinusitis with left orbital involvement from indolent mucormycosis. The patient was treated with aggressive systemic antifungal therapy, left retrobulbar injection of liposomal amphotericin B, reduction in immunosuppression, and conservative surgical debridement. Although the left olfactory cleft was involved, the cribriform plate was not resected due to risk of seeding the intracranial space. Given mild orbital involvement, no orbital debridement was performed and the patient had resolution of his orbital findings with systemic and retrobulbar amphotericin B. The patient had clinical and radiographic stability at 6-month follow-up.
Conclusions: Conservative resection with subsequent long-term antifungal treatment can be a successful regimen in indolent mucormycosis. Retrobulbar amphotericin B may be a prudent orbit-sparing adjuvant therapy in indolent mucormycosis.
Keywords: Chronic invasive fungal sinusitis; Conservative debridement; Fungal orbital cellulitis; IFS, Invasive Fungal Sinusitis; Indolent mucormycosis; TRAMB, transcutaneous retrobulbar injection of amphotericin B; Transcutaneous retrobulbar injection of amphotericin B.
© 2022 Published by Elsevier Inc.
Conflict of interest statement
The authors have no relevant financial disclosures.
Figures
References
-
- Mignogna M.D., Fortuna G., Leuci S., et al. Mucormycosis in immunocompetent patients: a case-series of patients with maxillary sinus involvement and a critical review of the literature. Int J Infect Dis. 2011;15(8):e533–e540. - PubMed
-
- Finn D.G., Farmer J.C. Chronic mucormycosis. Laryngoscope. 1982;92(7 Pt 1):761–766. - PubMed
-
- Kalin-Hajdu E., Hirabayashi K.E., Vagefi M.R., Kersten R.C. Invasive fungal sinusitis: treatment of the orbit. Curr Opin Ophthalmol. 2017;28(5):522–533. - PubMed
-
- Hirabayashi K.E., Kalin-Hajdu E., Brodie F.L., et al. Retrobulbar injection of amphotericin B for orbital mucormycosis. Ophthalmic Plast Reconstr Surg. 2017;33(4):e94–e97. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
