

Paediatric intracranial dural arteriovenous shunts: types, clinical presentation and therapeutic management
- PMID: 35243346
- PMCID: PMC8889109
- DOI: 10.1093/braincomms/fcac043
Paediatric intracranial dural arteriovenous shunts: types, clinical presentation and therapeutic management
Abstract
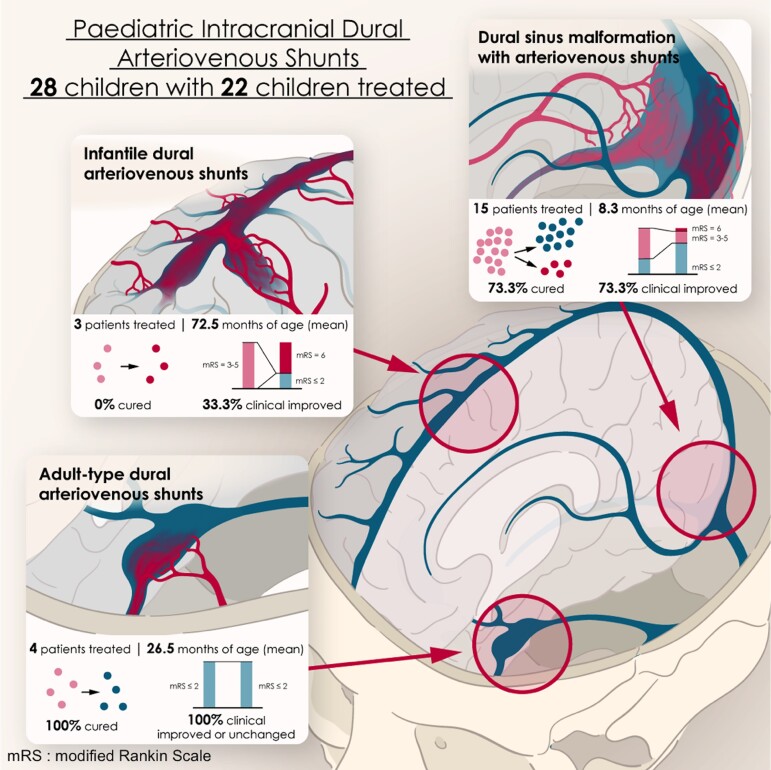
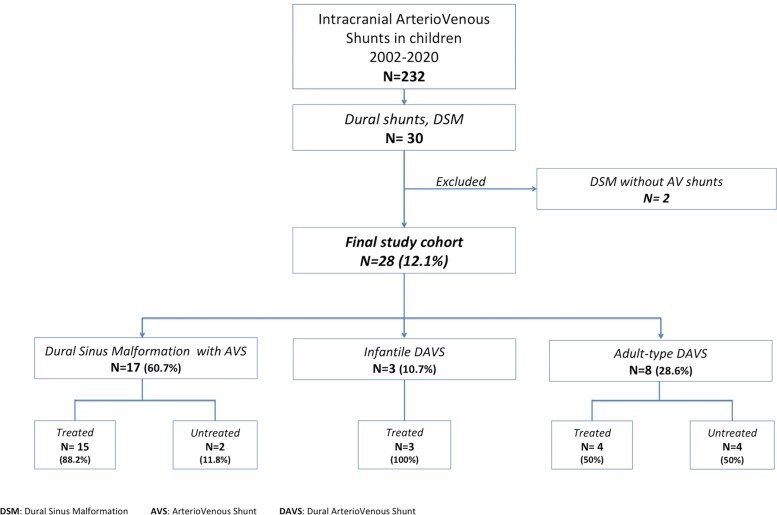
Paediatric intracranial dural arteriovenous shunts have clinical presentations and evolutions, with angiographic characteristics that differ from those described in adults. We report our experience concerning their therapeutic management, emphasizing the relevance of early diagnosis and appropriate treatment for satisfactory neurocognitive development. Using a prospective database, we reviewed the clinical and radiological data of all children with dural arteriovenous shunts managed between 2002 and 2020. Dural shunts were categorized into three types: dural sinus malformations with arteriovenous shunts; infantile dural arteriovenous shunts; and adult-type dural arteriovenous shunts. Therapeutic strategies and outcomes were analysed depending on lesional subtypes. Modified Rankin Scale for the paediatric population was assessed pre-treatment and at last follow-up. Twenty-eight patients [16 girls (57.1%); 12 boys (42.9%)] were included: 17 dural sinus malformation [10 boys (58.8%); seven girls (41.2%)], three infantile shunts [three girls (100%)], eight adult-type shunts [four girls (50%)]; four boys (50%)], with a mean age of 19.2 ± 36.6 months at presentation. Twelve (42.9%) had a modified Rankin Scale score of 0-2, four (14.3%) had a score of 3, three (10.7%) had a score of 4 and eight (28.6%) had a score of 5. Embolization was performed in 22 children [78.6%; 12 girls (54.5%); 10 boys (45.5%)]. Fifteen patients could be cured (68.2%): 11 dural sinus malformations (73.3%), four adult-type lesions (100%) but no infantile shunt. Mean post-treatment follow-up was 39.5 months (max. 139 months): 14 patients (63.6%) presented a modified Rankin Scale score of 0-2 and eight (36.4%) had a score ≥3. In the dural sinus malformation group, the modified Rankin Scale score was improved in 11 patients (73.3%) and unchanged in three (20%). Only one patient with infantile subtype (33.3%) improved clinically. In the adult-subtype group, all children (100%) improved. Of six untreated patients [four girls (66.7%); two boys (33.3%)], four with adult-subtype shunts showed uneventful evolutions, one with dural sinus malformation died, and therapeutic abortion was conducted in an antenatally diagnosed dural sinus malformation. Paediatric dural fistulas comprise different subtypes with variable clinical courses. Proper diagnosis is mandatory for optimal therapeutic strategies within appropriate therapeutic windows.
Keywords: congenital; dural shunts; fistula; paediatrics; vascular malformation.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures

References
-
- Hetts SW, Moftakhar P, Maluste N, et al. Pediatric intracranial dural arteriovenous fistulas: Age-related differences in clinical features, angioarchitecture, and treatment outcomes. J Neurosurg Pediatr. 2016;18:602–610. - PubMed
-
- Garcia-Monaco R, Rodesch G, Terbrugge K, Burrows P, Lasjaunias P. Multifocal dural arteriovenous shunts in children. Childs Nerv Syst. 1991;7:425–431. - PubMed
-
- Lasjaunias P, Magufis G, Goulao A, et al. Anatomoclinical aspects of dural arteriovenous shunts in children. Review of 29 cases. Interv Neuroradiol. 1996;2:179–191. - PubMed
-
- Sanchez-Mejia RO, Chennupati SK, Gupta N, Fullerton H, Young WL, Lawton MT. Superior outcomes in children compared with adults after microsurgical resection of brain arteriovenous malformations. J Neurosurg. 2006;105(2 Suppl):82–85. - PubMed
LinkOut - more resources
Full Text Sources