

Dose-limiting, adverse event-associated bradycardia with β-blocker treatment of atrial fibrillation in the GENETIC-AF trial
- PMID: 35243434
- PMCID: PMC8859785
- DOI: 10.1016/j.hroo.2021.11.005
Dose-limiting, adverse event-associated bradycardia with β-blocker treatment of atrial fibrillation in the GENETIC-AF trial
Abstract
Background: Heart failure (HF) patients with atrial fibrillation (AF) often have conduction system disorders, which may be worsened by β-blocker therapy.
Objective: In a post hoc analysis we examined the prevalence of bradycardia and its association with adverse events (AEs) and failure to achieve target dose in the GENETIC-AF trial.
Methods: Patients randomized to metoprolol (n = 125) or bucindolol (n = 131) entering 24-week efficacy follow-up and receiving study medication were evaluated. Bradycardia was defined as an electrocardiogram (ECG) heart rate (HR) <60 beats per minute (bpm) and severe bradycardia <50 bpm.
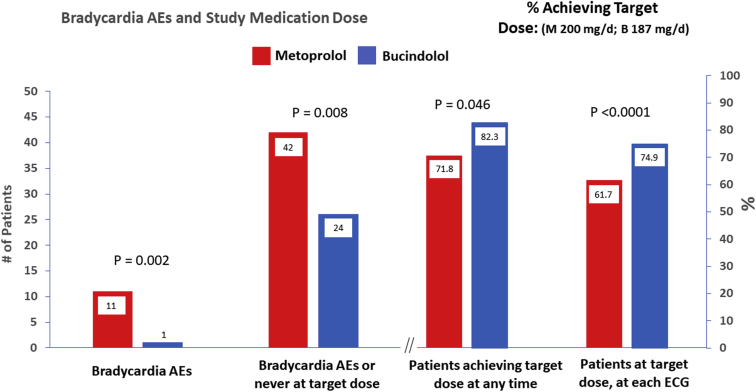
Results: Mean HR in sinus rhythm (SR) was 62.6 ± 12.5 bpm for metoprolol and 68.3 ± 11.1 bpm for bucindolol (P < .0001), but in AF HRs were not different (87.5 bpm vs 89.7 bpm, respectively). Episodes per patient for bucindolol vs metoprolol were 0.82 vs 2.08 (P < .001) for bradycardia and 0.24 vs 0.57 for severe bradycardia (P < .001), with 98.9% of the episodes occurring in SR. Patients experiencing bradycardia had a 4.15-fold higher prevalence of study medication dose reduction (P <.0001) compared to patients without bradycardia. Fewer patients receiving metoprolol were at target dose (61.7% vs 74.9% for bucindolol, P < .0001) at ECG recordings, and bradycardia AEs were more prevalent in the metoprolol group (13 vs 1 for bucindolol, P = .001). On multivariate analysis of 21 candidate bradycardia predictors including presence of a device with pacing capability, bucindolol treatment was associated with the greatest degree of prevention (Zodds ratio -4.24, P < .0001).
Conclusion: In AF-prone HF patients bradycardia may limit the effectiveness of β blockers, and this property is agent-dependent.
Keywords: Atrial fibrillation; Beta blockers; Bradyarrhythmias; Heart failure; Pharmacogenetics.
© 2021 Heart Rhythm Society. Published by Elsevier Inc.
Figures



References
-
- Wang T.J., Larson M.G., Levy D., et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107:2920–2925. - PubMed
-
- Bristow M.R. Treatment of chronic heart failure with β-adrenergic receptor antagonists: a convergence of receptor pharmacology and clinical cardiology. Circ Res. 2011;109:1176–1194. - PubMed
-
- Van Veldhuisen D.J., Aass H., El Allaf D., et al. Presence and development of atrial fibrillation in chronic heart failure. Experiences from the MERIT-HF Study. Eur J Heart Fail. 2006;8:539–546. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
