

Five Year Outcomes in Patients with End Stage Renal Disease Who Received a Bioengineered Human Acellular Vessel for Dialysis Access
- PMID: 35243473
- PMCID: PMC8881722
- DOI: 10.1016/j.ejvsvf.2022.01.003
Five Year Outcomes in Patients with End Stage Renal Disease Who Received a Bioengineered Human Acellular Vessel for Dialysis Access
Abstract
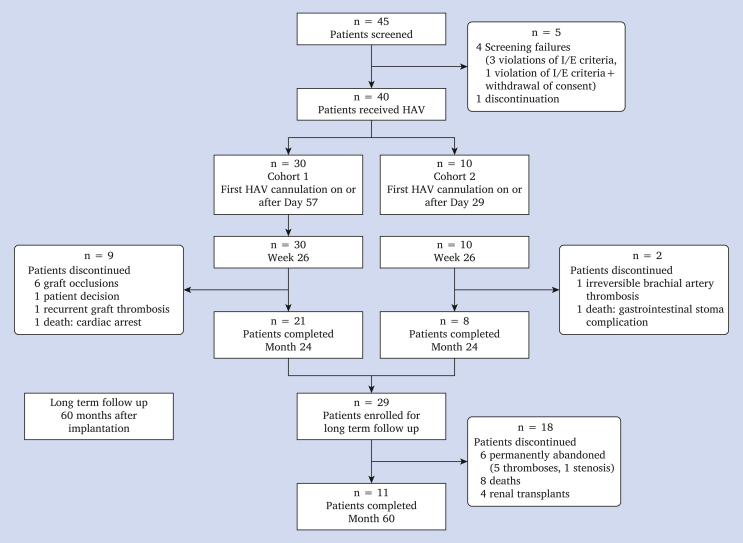
Objective: Patients with end stage renal failure who require haemodialysis suffer morbidity and mortality due to vascular access. Bioengineered human acellular vessels (HAVs) may provide a haemodialysis access option with fewer complications than other grafts. In a prospective phase II trial from 2012 to 2014 (NCT01744418), HAVs were implanted into 40 haemodialysis patients at three sites in Poland. The trial protocol for this "first in man" use of the HAV contemplated only two years of follow up, and the trial results were initially reported in 2016. In light of the retained HAV function seen in many of the patients at the two year time point, follow up for patients who were still alive was extended to a total of 10 years. This interim follow up report, at the long term time point of five years, assessed patient and conduit status in those who continued routine dialysis with the HAV.
Methods: HAVs are bioengineered by culturing human vascular smooth muscle cells on a biodegradable polymer matrix. In this study, patients with patent HAV implants at 24 months were followed every three months, starting at month 27 through to month 60, or at least five years post-implantation. This report contains the follow up functional and histological data on 29 of the original 40 patients who demonstrated HAV function at the 24 month time point.
Results: Eleven patients completed at month 60. One patient maintained primary patency, and 10 maintained secondary patency. Secondary patency was estimated at 58.2% (95% confidence interval 39.2-73.1) at five years, after censoring for deaths (n = 8) and withdrawals (n = 1). No HAV conduit infections were reported during the follow up period.
Conclusion: This phase II long term follow up shows that the human acellular vessel (HAV) may provide durable and functional haemodialysis access for patients with end stage renal disease.
Keywords: Blood vessel prosthesis; Haemodialysis; Regenerative medicine; Tissue engineering; Vascular access.
© 2022 The Authors.
Figures

References
-
- Almasri J., Alsawas M., Mainou M., Mustafa R.A., Wang Z., Woo K., et al. Outcomes of vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg. 2016;64:236–243. - PubMed
-
- Akoh J.A., Patel N. Infection of hemodialysis arteriovenous grafts. J Vasc Access. 2010;11:155–158. - PubMed
-
- Katzman H.E., Glickman M.H., Schild A.F., Fujitani R.M., Lawson J.H. Multicenter evaluation of the bovine mesenteric vein bioprostheses for hemodialysis access in patients with an earlier failed prosthetic graft. J Am Coll Surg. 2005;201:223–230. - PubMed
-
- Arhuidese I., Orandi B., Nejim B., Malas M. Utilization, patency, and complications associated with vascular access for hemodialysis in the United States. J Vasc Surg. 2018;68:1166–1174. - PubMed
-
- Beathard G.A. The treatment of vascular access graft dysfunction: a nephrologist's view and experience. Adv Ren Replace Ther. 1994;1:131–147. - PubMed
LinkOut - more resources
Full Text Sources