

Hashimoto thyroiditis: an evidence-based guide to etiology, diagnosis and treatment
- PMID: 35243857
- PMCID: PMC9478900
- DOI: 10.20452/pamw.16222
Hashimoto thyroiditis: an evidence-based guide to etiology, diagnosis and treatment
Abstract
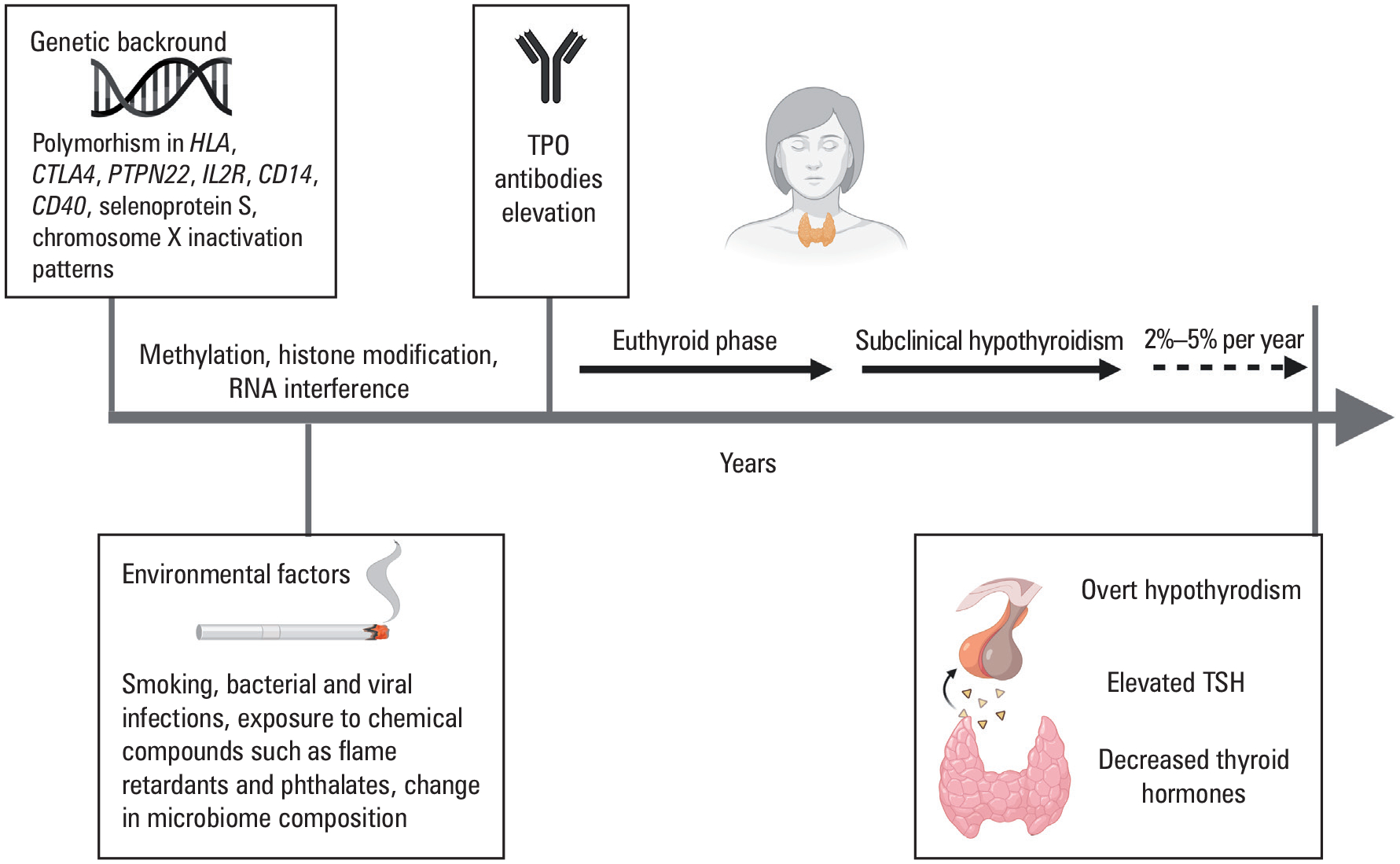
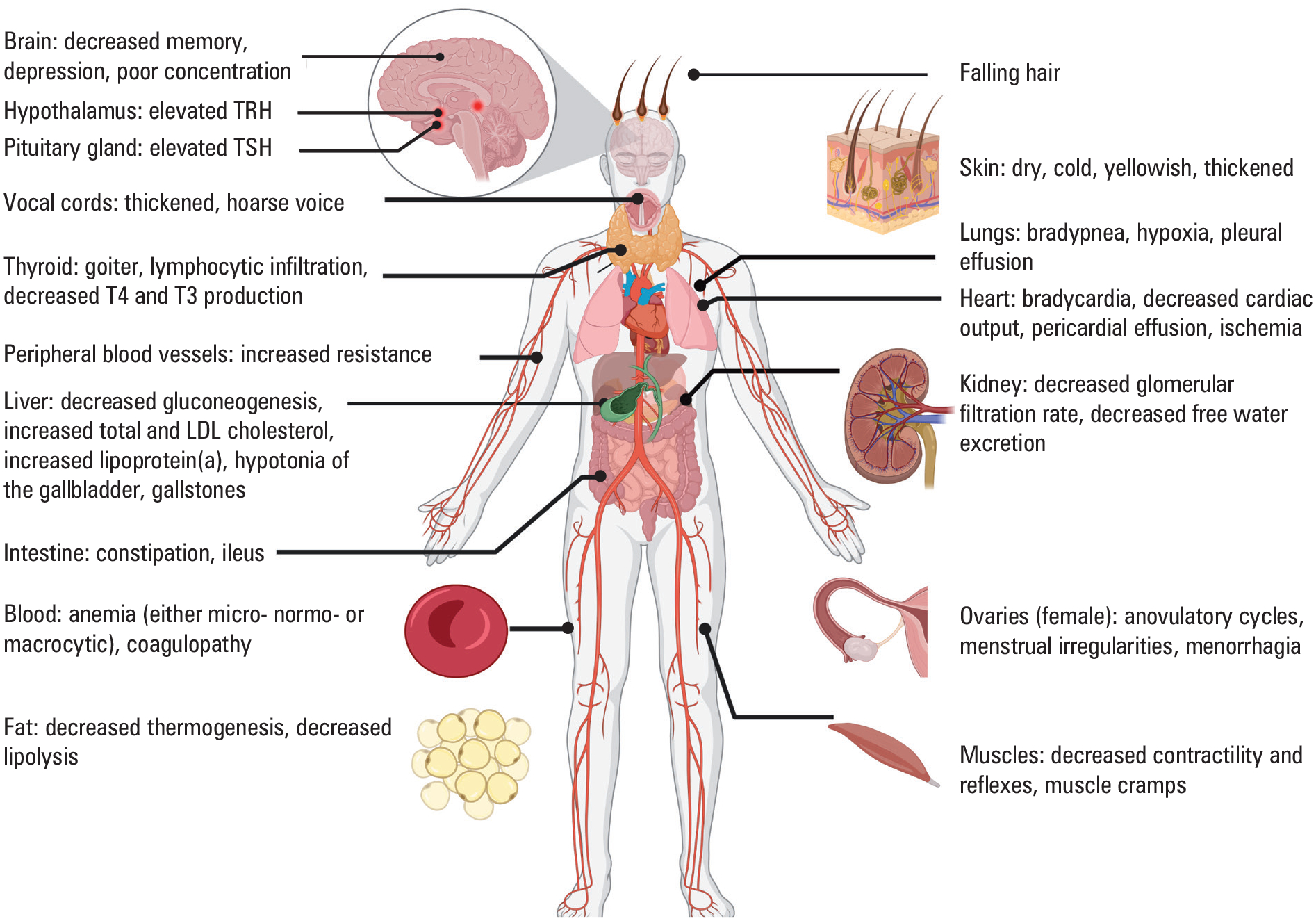
Hashimoto thyroiditis (HT) is a common autoimmune disorder, affecting women 7-10 times more often than men, that develops because of genetic susceptibility, Xchromosome inactivation patterns modulated by environmental factors as well as microbiome composition, and leads to an imbalance in self‑tolerance mechanisms. The consequential thyroid infiltration by lymphocytes, potentiated by antibody‑mediated autoimmune response through the antibodies against thyroid peroxidase (TPOAbs), leads to a destruction of thyrocytes. The presence of TPOAbs is associated with a 2 to 4‑fold increase in the risk of recurrent miscarriages and preterm birth in pregnant women. The clinical presentation of HT includes: (A) thyrotoxicosis, when stored thyroid hormones are released to circulation from destroyed thyroid follicles; (B) euthyroidism, when preserved thyroid tissue compensates for destroyed thyrocytes; and (C) hypothyroidism, when thyroid hormone production by the affected thyroid gland is insufficient. The management of Hashitoxicosis is based on symptoms control usually with β‑blockers, euthyroidism requires periodical thyroid stimulating hormone measurements to assess for progression to hypothyroidism, and hypothyroidism is treated with thyroid hormone replacement therapy. The dose of levothyroxine (LT4) used for treatment is based on the degree of preserved thyroid functionality and lean body mass, and usually ranges from 1.4 to 1.8 mcg/kg/day. There is insufficient evidence to recommend for or against therapy with triiodothyronine (T3), apart from in pregnancy when only levothyroxine is indicated, as T3 does not sufficiently cross fetal blood‑brain barrier. HT is associated with 1.6 times higher risk of papillary thyroid cancer and 60 times higher risk of thyroid lymphoma than in general the population.
Conflict of interest statement
Figures
References
-
- Hashimoto H The knowledge of the lymphomatous changes in the thyroid gland (struma lymphomatosa) [in German]. Archiv für klinische Chirurgie. 1912; 97: 219.
-
- Ralli M, Angeletti D, Fiore M, et al. Hashimoto’s thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev. 2020; 19: 102649. - PubMed
-
- McLeod DS, Caturegli P, Cooper DS, et al. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. JAMA. 2014; 311: 1563–1565. - PubMed
-
- Song RH, Yao QM, Wang B, et al. Thyroid disorders in patients with myasthenia gravis: a systematic review and meta-analysis. Autoimmun Rev. 2019; 18: 102368. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical