

Effect of Time to Treatment With Antiarrhythmic Drugs on Return of Spontaneous Circulation in Shock-Refractory Out-of-Hospital Cardiac Arrest
- PMID: 35243875
- PMCID: PMC9075276
- DOI: 10.1161/JAHA.121.023958
Effect of Time to Treatment With Antiarrhythmic Drugs on Return of Spontaneous Circulation in Shock-Refractory Out-of-Hospital Cardiac Arrest
Abstract
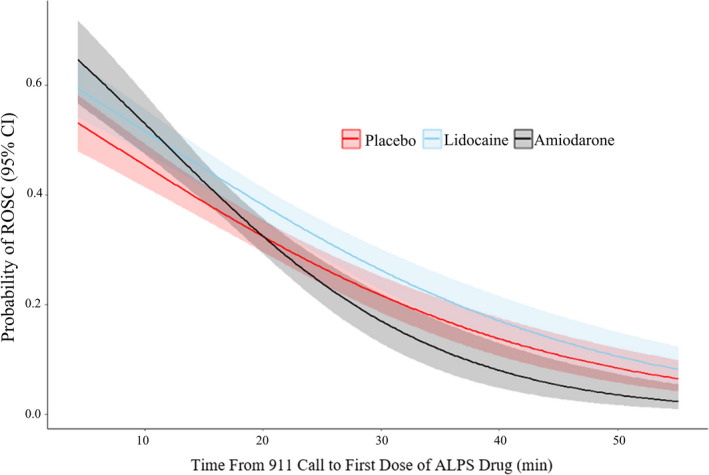
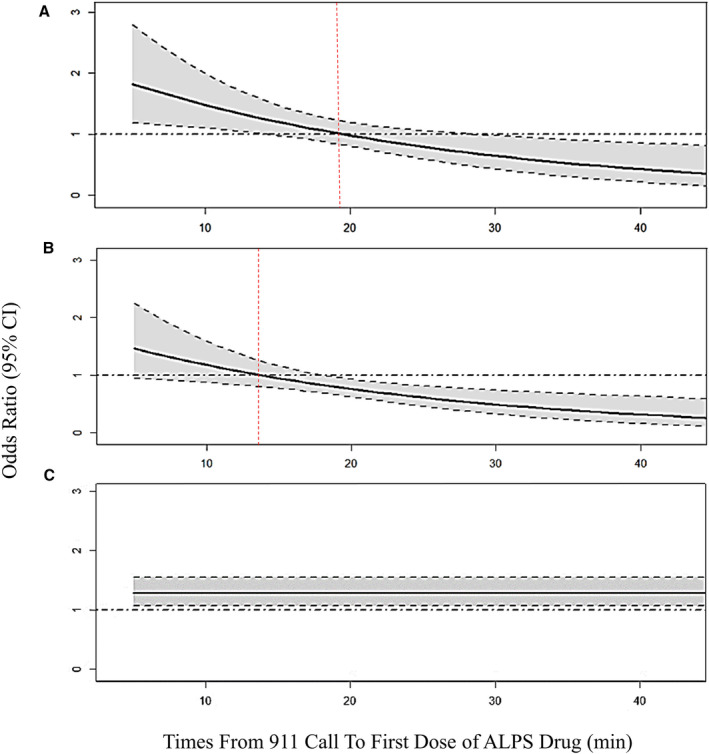
Background The effects of amiodarone and lidocaine on the return of spontaneous circulation (ROSC) in relation to time to treatment in patients with out-of-hospital cardiac arrest is not known. We conducted a post hoc analysis of the ROC ALPS (Resuscitation Outcomes Consortium Amiodarone, Lidocaine, Placebo) randomized controlled trial examining the association of time to treatment (drug or placebo) with ROSC at hospital arrival. Methods and Results In the trial, adults with nontraumatic out-of-hospital cardiac arrest with initial refractory ventricular fibrillation or pulseless ventricular tachycardia after at least 1 defibrillation were randomly assigned to receive amiodarone, lidocaine, or placebo. We used logistic regression to examine the association of time to treatment (911 call to study drug administration) with ROSC. An interaction term between treatment and time to treatment was included to determine the potential effect of time on treatment effects. Overall, 1112 (36.7%) patients had ROSC at hospital arrival (350 in the amiodarone arm, 396 in the lidocaine arm, and 366 in the placebo arm). The proportion of patients who had ROSC decreased as time to drug administration increased, in patients treated with amiodarone (odds ratio, 0.92; 95% CI, 0.90-0.94 per minute increase), lidocaine (odds ratio, 0.95; 95% CI, 0.93-0.96), and placebo (odds ratio, 0.95; 95% CI, 0.93-0.96). With shorter times to drug administration, the proportion with ROSC was higher in amiodarone versus placebo recipients. Conclusions The probability of ROSC decreased as time to drug administration increased. The effect of amiodarone but not lidocaine to restore ROSC declined with longer times to drug administration, potentially attributable to its adverse hemodynamic effects.
Keywords: amiodarone; lidocaine; out‐of‐hospital cardiac arrest; return of spontaneous circulation.
Figures
References
-
- Deyell MW, AbdelWahab A, Angaran P, Essebag V, Glover B, Gula LJ, Khoo C, Lane C, Nault I, Nery PB, et al. 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society Position Statement on the management of ventricular tachycardia and fibrillation in patients with structural heart disease. Can J Cardiol. 2020;36:822–836. doi: 10.1016/j.cjca.2020.04.004 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
