

Increased Circulating Endothelin 1 Is Associated With Postoperative Hypoxemia in Infants With Single-Ventricle Heart Disease Undergoing Superior Cavopulmonary Anastomosis
- PMID: 35243904
- PMCID: PMC9075322
- DOI: 10.1161/JAHA.121.024007
Increased Circulating Endothelin 1 Is Associated With Postoperative Hypoxemia in Infants With Single-Ventricle Heart Disease Undergoing Superior Cavopulmonary Anastomosis
Abstract
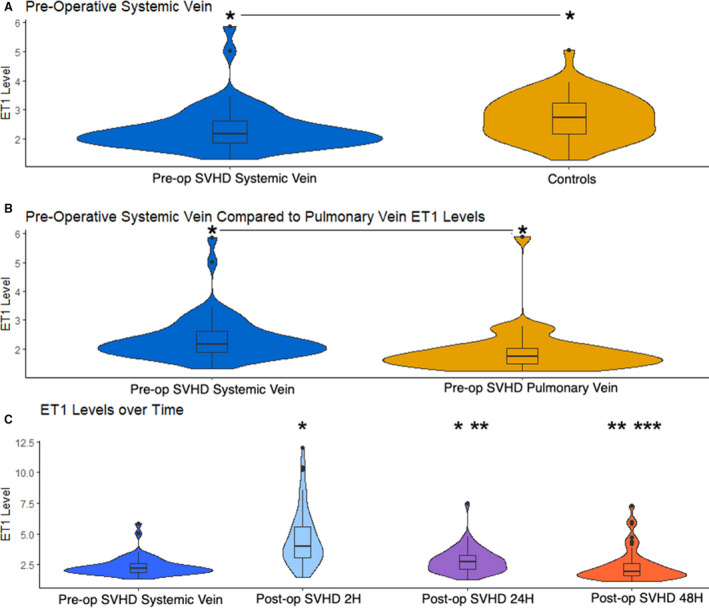
Background Inadequate pulmonary vascular growth results in morbidity for many children with single-ventricle heart disease (SVHD). Endothelin 1 (ET1) is a potent vasoconstrictor and stimulator of pulmonary artery smooth muscle proliferation. Circulating ET1 levels and their association with outcomes have not been studied during early SVHD palliation. We aimed to define circulating levels of ET1 in patients with SVHD undergoing stage 2 palliation and evaluate their relationship to postoperative hypoxemia. We hypothesized that patients with SVHD with higher ET1 concentration would have a greater post-stage 2 hypoxemia. Methods and Results Prospective cohort study of 55 subjects with SVHD undergoing stage 2 palliation and 50 controls. Samples for ET1 analysis were collected at preoperation (systemic and pulmonary vein) and 2, 24, and 48 hours postoperation for cases and a single time point for controls. The primary outcome was percentage of first 48 postoperative hours with clinically significant hypoxemia (saturation, <70%). ET1 concentration was lower in preoperative cases than controls (2.2 versus 2.7 pg/mL; P=0.0015) and in the pulmonary vein than systemic vein (1.7 versus 2.2 pg/mL; P<0.001). ET1 level increased by 2 hours postoperation and trended back to baseline by 48 hours. Higher preoperative pulmonary vein ET1 and 2 hours postoperative ET1 were associated with larger hypoxemia burden (10.6% versus 2.7% [P=0.0081]; and 7.6% versus 3.2% [P=0.01], respectively). Multivariable testing demonstrated ET1 concentration and cardiopulmonary bypass time were associated with hypoxemia, whereas catheterization measurements and clinical variables were not. Conclusions Infants with SVHD with higher perioperative ET1 concentration experience more post-stage 2 hypoxemia. ET1 activity may be a modifiable risk factor of pulmonary vascular inadequacy for stage 2 palliation.
Keywords: Glenn operation; biomarkers; endothelin 1; hypoxemia; single‐ventricle palliation.
Figures
Similar articles
-
Increased Endothelin-1 Is Associated With Morbidity in Single Ventricle Heart Disease in Children Undergoing Fontan Palliation.JACC Adv. 2025 Apr;4(4):101672. doi: 10.1016/j.jacadv.2025.101672. Epub 2025 Mar 20. JACC Adv. 2025. PMID: 40117690 Free PMC article.
-
Arginine-NO metabolites are associated with morbidity in single ventricle infants undergoing stage 2 palliation.Pediatr Res. 2024 Jul;96(2):347-355. doi: 10.1038/s41390-024-03162-y. Epub 2024 Apr 2. Pediatr Res. 2024. PMID: 38565916 Free PMC article.
-
Proteomic profiling identifies key differences between inter-stage infants with single ventricle heart disease and healthy controls.Transl Res. 2021 Mar;229:24-37. doi: 10.1016/j.trsl.2020.10.001. Epub 2020 Oct 9. Transl Res. 2021. PMID: 33045409 Free PMC article.
-
Arteriovenous fistula creation for hypoxia after single ventricle palliation: A single-institution experience and literature review.Congenit Heart Dis. 2019 Nov;14(6):1199-1206. doi: 10.1111/chd.12828. Epub 2019 Aug 1. Congenit Heart Dis. 2019. PMID: 31368206 Review.
-
Role of systemic to pulmonary artery shunt after cavopulmonary anastomosis.J Card Surg. 2013 Sep;28(5):599-603. doi: 10.1111/jocs.12154. Epub 2013 Jul 28. J Card Surg. 2013. PMID: 23889551 Review.
Cited by
-
Interstage Single Ventricle Heart Disease Infants Show Dysregulation in Multiple Metabolic Pathways: Targeted Metabolomics Analysis.JACC Adv. 2023 Jan;2(1):100169. doi: 10.1016/j.jacadv.2022.100169. Epub 2023 Jan 27. JACC Adv. 2023. PMID: 36875009 Free PMC article.
-
Circulating biomarkers of extracellular matrix dysregulation are associated with adverse post-stage 2 outcomes in infants with single ventricle heart disease.Sci Rep. 2023 Sep 28;13(1):16318. doi: 10.1038/s41598-023-43562-4. Sci Rep. 2023. PMID: 37770592 Free PMC article.
-
Metabolomics in Single Ventricle Heart Disease: Glimpsing the Pathobiology of Stage 2 Palliation.JACC Adv. 2023 Jan 27;2(1):100170. doi: 10.1016/j.jacadv.2022.100170. eCollection 2023 Jan. JACC Adv. 2023. PMID: 38939018 Free PMC article.
-
Increased Endothelin-1 Is Associated With Morbidity in Single Ventricle Heart Disease in Children Undergoing Fontan Palliation.JACC Adv. 2025 Apr;4(4):101672. doi: 10.1016/j.jacadv.2025.101672. Epub 2025 Mar 20. JACC Adv. 2025. PMID: 40117690 Free PMC article.
References
-
- Brown DW, Gauvreau K, Powell AJ, Lang P, del Nido PJ, Odegard KC, Geva T. Cardiac magnetic resonance versus routine cardiac catheterization before bidirectional Glenn anastomosis: long‐term follow‐up of a prospective randomized trial. J Thorac Cardiovasc Surg. 2013;146:1172–1178. doi: 10.1016/j.jtcvs.2012.12.079 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
