

Endocarditis-associated rapidly progressive glomerulonephritis mimicking vasculitis: a diagnostic and treatment challenge
- PMID: 35243934
- PMCID: PMC8903796
- DOI: 10.1080/07853890.2022.2046288
Endocarditis-associated rapidly progressive glomerulonephritis mimicking vasculitis: a diagnostic and treatment challenge
Abstract
Background: Infective endocarditis (IE)-associated rapidly progressive glomerulonephritis (RPGN) is rarely reported. Sporadic case reports have noted the diagnostic and therapeutic challenge in IE-associated glomerulonephritis because it may masquerade as idiopathic vasculitis.
Methods: Patients with clinical diagnosis of IE-related RPGN in a tertiary hospital in China between January 2004 and May 2021 were identified and retrospectively reviewed.
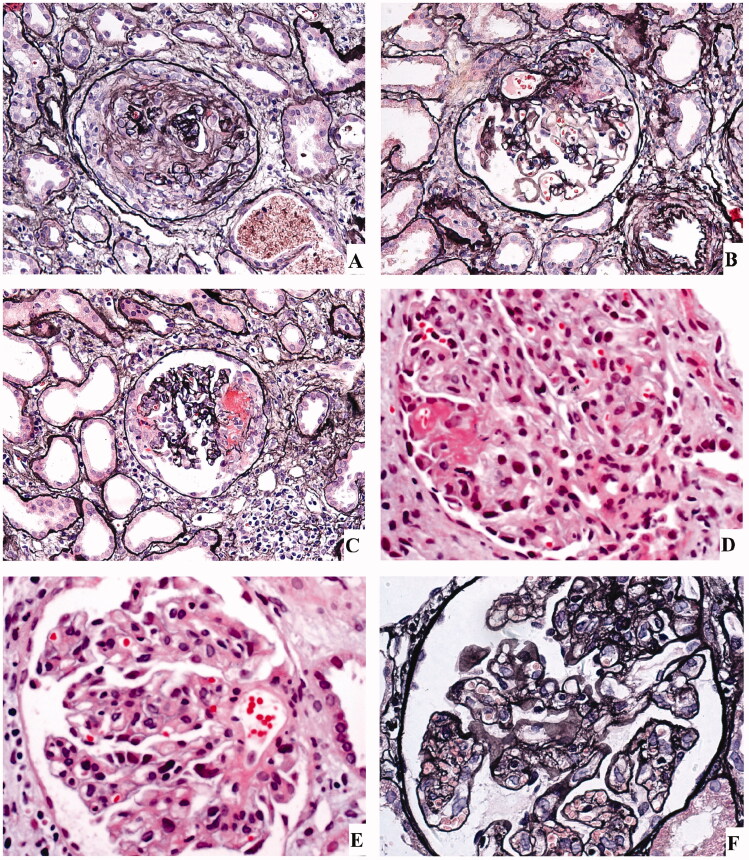
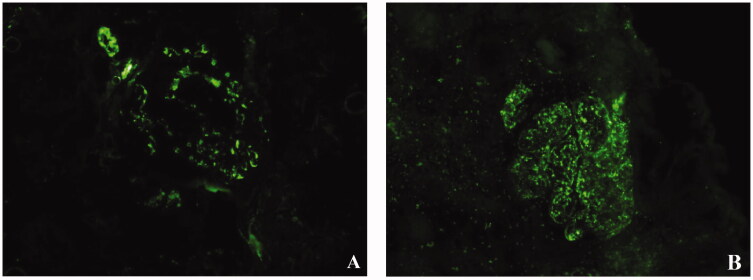
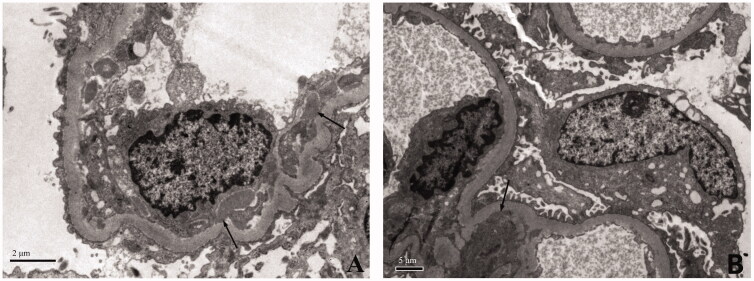
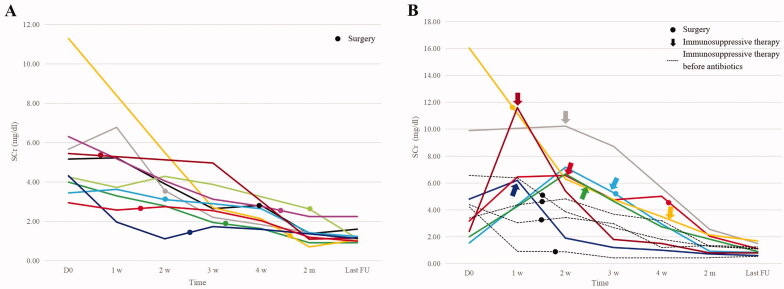
Results: Twenty-four patients with IE-associated RPGN were identified. All patients presented with fever and multiorgan system involvement on top of heart and kidneys, spleen (79%, 19/24), skin (63%, 15/24), lung (33%, 8/24) and nervous system (17%, 4/24). Six of the 24 patients (25%) were initially suspected to have ANCA-associated or IgA vasculitis. Forty-five percent of patients are seropositive for ANCA. Renal histology showed mesangial and/or endocapillary hypercellularity with extensive crescents in most patients. C3-dominant deposition was the predominant pattern on immunofluorescence and pauci-immune necrotising crescentic glomerulonephritis was observed in one case. All patients received antibiotics with or without surgery. Six patients received immunosuppressive therapy before antibiotics due to misdiagnosis and seven patients received immunosuppressive therapy after antibiotics due to persistence of renal failure. Three of the 24 patients died due to severe infection. All the surviving patients had partial or complete recovery of renal function.
Conclusion: IE-associated RPGN is rare and the differential diagnosis from idiopathic vasculitis can be challenging due to overlaps in clinical manifestations, ANCA positivity and absence of typical presentations of IE. The prognosis is generally good if antibiotics and surgery are not delayed. The decision on introducing immunoruppressive treatment should be made carefully on a case by case basis when kidney function does not improve appropriately after proper anti-infective therapy.Key messagesInfective endocarditis associated RPGN is rare and differentiating it from idiopathic vasculitis can be challenging due to overlap in clinical manifestations, ANCA positivity and occasional absence of typical manifestations of infective endocarditis.Kidney function usually responds to antibiotic therapy alone.Immunosuppressive therapy may be beneficial in carefully selected patients whose kidney function does not improve with antibiotics alone.
Keywords: Infective endocarditis; RPGN; immunosuppressive therapy; vasculitis.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Infective Endocarditis-Associated Purpura and Glomerulonephritis Mimicking IgA Vasculitis: A Diagnostic Pitfall.Am J Med. 2021 Dec;134(12):1539-1545.e1. doi: 10.1016/j.amjmed.2021.06.033. Epub 2021 Jul 31. Am J Med. 2021. PMID: 34343512
-
[The relationships of rapidly progressive glomerulonephritis (RPGN), crescentic glomerulonephritis and vasculitis: the clinical, histopathological and therapeutic considerations].Rev Med Chir Soc Med Nat Iasi. 1996 Jul-Dec;100(3-4):63-72. Rev Med Chir Soc Med Nat Iasi. 1996. PMID: 9455438 Romanian.
-
Antineutrophil cytoplasmic antibody-positive infective endocarditis complicated by acute kidney injury: a case report and literature review.J Int Med Res. 2020 Oct;48(10):300060520963990. doi: 10.1177/0300060520963990. J Int Med Res. 2020. PMID: 33078666 Free PMC article. Review.
-
Vasculitides and glomerulonephritis associated with Staphylocococcus aureus infective endocarditis: cases reports and mini-review of the literature.Ann Med. 2020 Sep;52(6):265-274. doi: 10.1080/07853890.2020.1778778. Epub 2020 Jun 26. Ann Med. 2020. PMID: 32588668 Free PMC article. Review.
-
[Idiopathic rapidly progressive glomerulonephritis and small vessel vasculitis].Zhonghua Nei Ke Za Zhi. 1997 Sep;36(9):603-6. Zhonghua Nei Ke Za Zhi. 1997. PMID: 10436970 Chinese.
Cited by
-
Native and prosthetic valve infective endocarditis complicated by rapidly progressive glomerulonephritis and its diagnostic challenges and therapeutic implications.Clin Case Rep. 2024 Jun 11;12(6):e9054. doi: 10.1002/ccr3.9054. eCollection 2024 Jun. Clin Case Rep. 2024. PMID: 38868123 Free PMC article.
-
Development of Palpable Purpura in a Patient With Infective Endocarditis: A Case Report.Cureus. 2024 Jul 1;16(7):e63601. doi: 10.7759/cureus.63601. eCollection 2024 Jul. Cureus. 2024. PMID: 39087182 Free PMC article.
-
Proteinase‑3‑antineutrophil cytoplasmic antibody‑associated vasculitis secondary to subacute infective endocarditis: A case report.Exp Ther Med. 2024 Mar 20;27(5):216. doi: 10.3892/etm.2024.12504. eCollection 2024 May. Exp Ther Med. 2024. PMID: 38590565 Free PMC article.
-
Immunosuppressant Use in Infective Endocarditis-Associated Glomerulonephritis: A Systematic Review.Clin Drug Investig. 2025 Aug;45(8):443-529. doi: 10.1007/s40261-025-01461-8. Epub 2025 Jul 19. Clin Drug Investig. 2025. PMID: 40682760 Free PMC article.
References
-
- Mahr A, Batteux F, Tubiana S, et al. ; IMAGE Study Group . Brief report: prevalence of antineutrophil cytoplasmic antibodies in infective endocarditis. Arthritis Rheumatol. 2014;66(6):1672–1677. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous